
 Jo Galvez
Jo Galvez
PF Digital Intake Forms | Eliminate Front Desk Data Entry
💡 Practice Fusion front desk data entry is one of the biggest time drains in small clinics. When a patient fills out a paper form, and staff have...
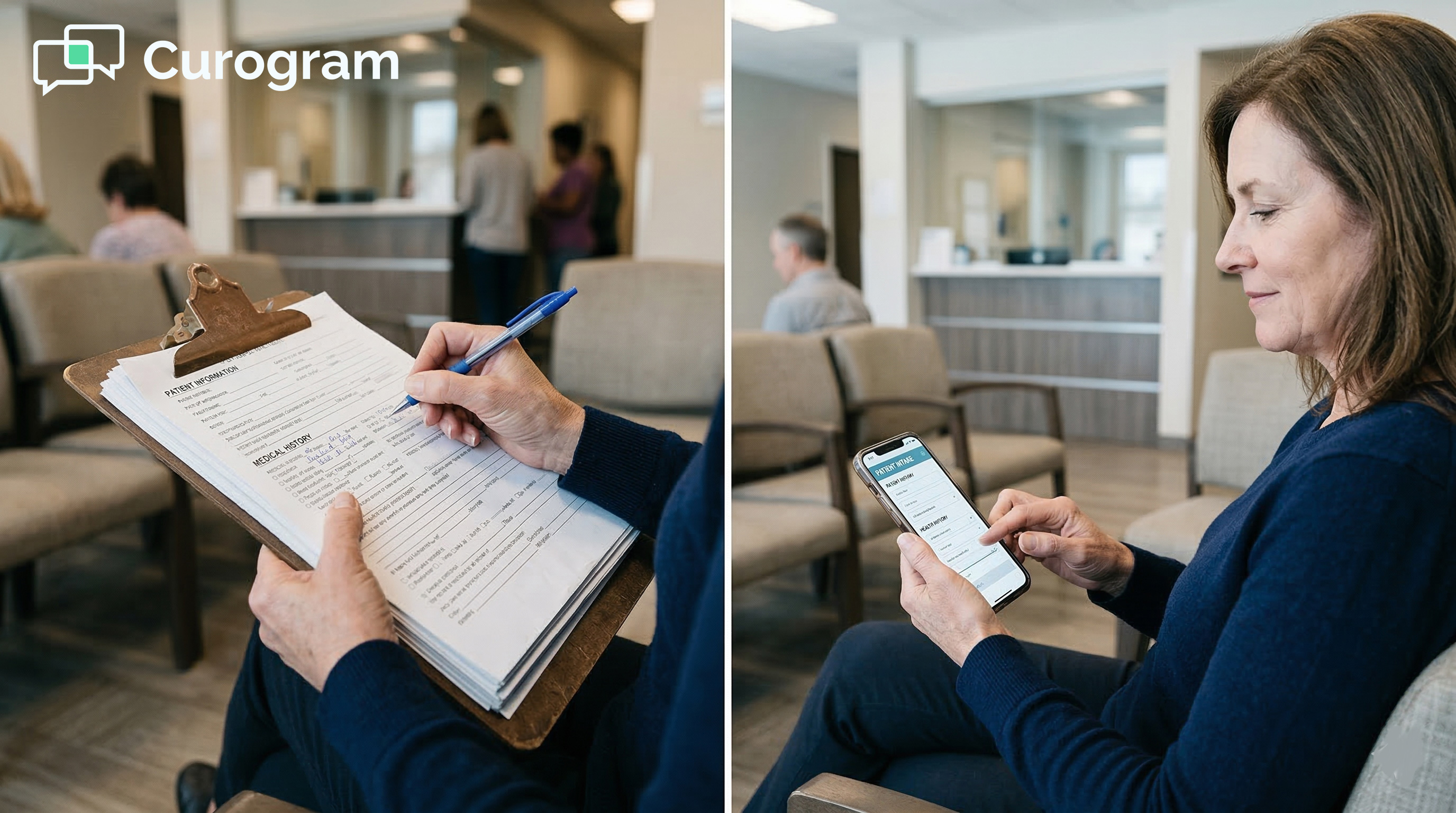
Your patients fill out forms on their phones every single day. Restaurant reservations. Insurance quotes. Bank applications.
But when they arrive at your Practice Fusion clinic, you hand them a clipboard with 19 pages.
It feels like a small thing. It is not. That clipboard costs your practice more time, money, and goodwill than most owners realize.
For small practices running Practice Fusion, the gap between what's possible and what's actually in place is wider than it should be.
Practice Fusion has a built-in Online Check-In tool. But most small clinics never use it fully. The setup is complex.
Patient adoption is low. The form data often ends up as a flat PDF that staff still have to re-type. So the paper stays.
This is the core problem: the same information gets recorded twice. The patient writes it. Staff types it. Every single visit.
Curogram's Text-to-Chart Pipeline is built to break that cycle. It sends patients a text link before their visit. They complete their intake on their phone.
That data writes directly into Practice Fusion chart notes, structured and ready. No re-entry needed.
This pillar covers everything small Practice Fusion clinics need to know: why paper intake persists, what the pipeline does, what it costs to stay on paper, how a real practice made the switch, and how to measure results.
Paper intake is not just an inconvenience. It is a daily drain on your staff, your schedule, and your charts. Understanding why most small Practice Fusion clinics still rely on paper is the first step toward fixing it.
Practice Fusion includes an Online Check-In feature. On paper, it should solve the problem. In reality, most small clinics with 1 to 5 providers do not use it at all, or barely use it. The reason is setup.
Configuring the tool requires technical steps that practices without IT staff struggle to complete. There is no one to call for help on a Tuesday morning when the front desk is already backed up.
Even when the feature is configured, patient adoption is the next wall. Patients need to log into a portal, use a specific browser, or click an email link they may have ignored.
The form does not feel like texting. It feels like a chore. So most patients skip it and show up ready to fill out paper instead.
Portal-based intake has one key flaw: it requires the patient to do something before they arrive that feels optional. Email links get buried. Portal logins get forgotten.
Based on our internal data, portal-based form completion rates at small Practice Fusion clinics often sit below 15%. That means 85% or more of patients still walk in without completing any pre-visit paperwork.
When most patients skip the digital option, the clinic cannot eliminate the paper fallback. So both systems run in parallel, which is actually worse. Staff must check the portal for the few who completed it, and hand clipboards to everyone else.
The standard new patient packet covers demographics, insurance information, medical history, current medications, allergies, consent forms, a HIPAA acknowledgment, and a financial responsibility agreement.
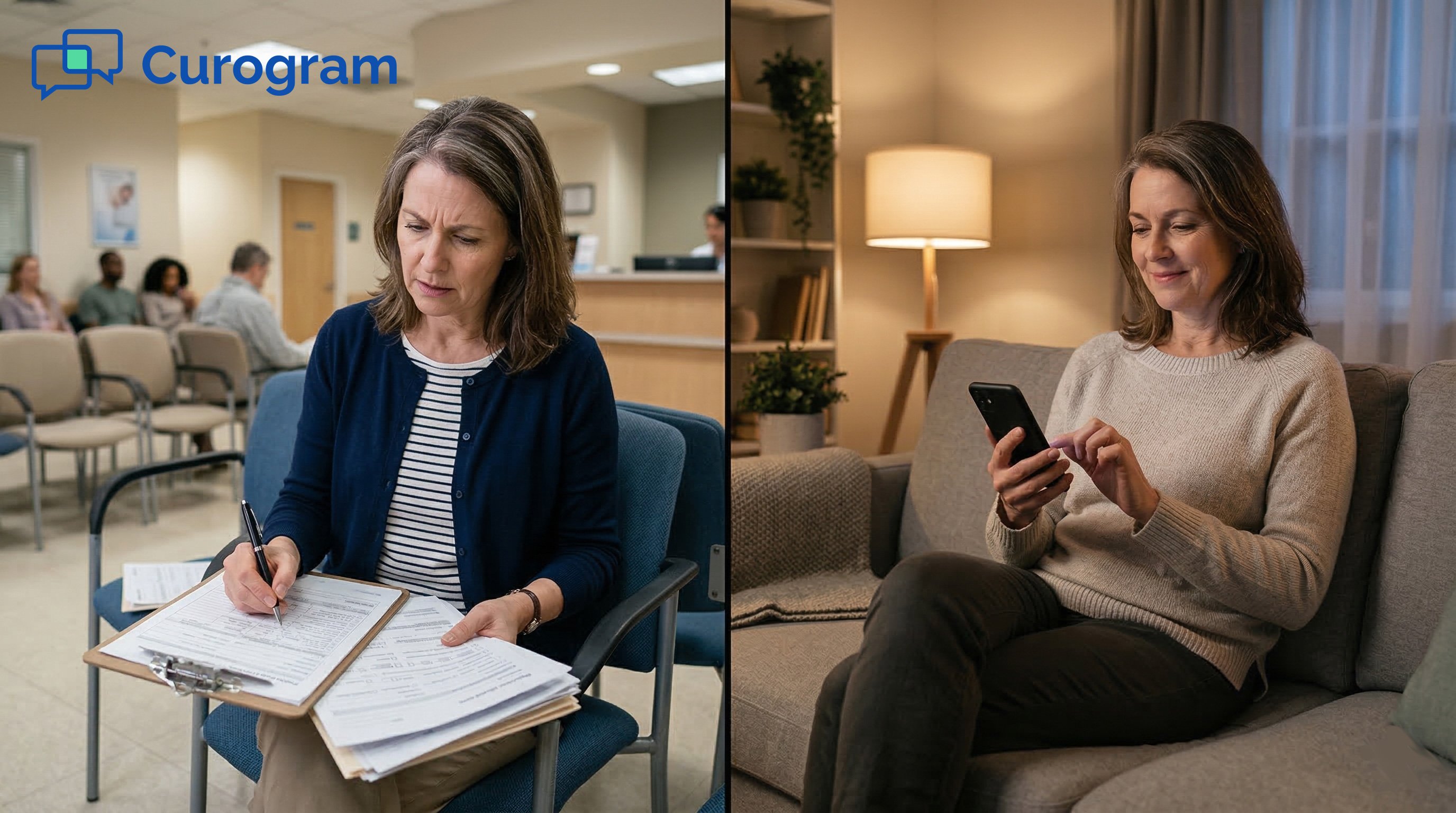
For specialty clinics, there are extra questionnaires on top. That stack can reach 15 to 19 pages. The patient fills it out in the waiting room. In 10-point font. With a pen that may or may not work.
Returning patients are not spared either. Annual forms, insurance updates, and medication reviews mean repeat paperwork every few visits.
The patient experience is identical to a visit five years ago, while their dentist down the street already sends them a text link.
After the patient is called back, a staff member picks up the paper form. They read it. They interpret the handwriting. They type each field into Practice Fusion.
This takes 10 to 15 minutes per patient. For a practice seeing 20 to 30 patients a day, that adds up to 3 to 7 or more hours of pure transcription work. Every day.
This is the double-entry trap: the practice does every piece of intake work twice. The patient writes it. Staff types it. Each step introduces room for error.
A misread medication name. A transposed phone number. An insurance ID that is one digit off.
These are not rare events. They are the predictable outcome of asking humans to copy handwriting under time pressure.
A wrong insurance ID leads to a denied claim. An incorrect phone number means a patient is unreachable for follow-up.
A misread allergy note becomes a clinical risk. The errors from paper intake do not stay in the waiting room. They travel downstream into billing, scheduling, and care delivery.
The cost of fixing these errors is real, even if it is hard to measure on a single bad day. Over time, transcription errors become a recurring tax on every department in the practice.
Curogram's Text-to-Chart Pipeline replaces every step of the paper intake process. The key is that it works through text messaging, which patients already use daily, with no app, no portal, and no extra friction.
Before the appointment, the patient gets a text from the practice's own number. The message is short and clear: please complete your intake forms before your visit, followed by a link.
The patient taps it. A mobile-optimized form opens in their phone's browser. There is no app to download and no account to create.
The form is designed for thumbs. Dropdowns, checkboxes, and auto-fill replace blank lines. Most patients complete it in under five minutes. They can do it at home, in the car, or in the parking lot before walking in.
One of the biggest barriers to digital intake adoption is asking patients to install something. Curogram's text-linked forms skip that entirely.
The link opens in the default mobile browser. It works on any smartphone. There is nothing to set up on the patient's end and no account to remember.
This matters most for older patients and those less comfortable with technology. If it opens when you tap a link, patients will use it. If it requires steps before you can even see the form, most will give up.
The form matches the practice's existing intake packet. Demographics, insurance details, medical history, medication list, allergies, consent forms, and HIPAA acknowledgment can all be included.
Fields are laid out for mobile screens. Required fields are clearly marked. The patient can complete and submit in one session without needing to print, sign, or scan anything.
Bilingual delivery is also supported. Practices serving diverse communities can send the form in the patient's preferred language. The data still writes back to Practice Fusion in the format the practice needs.
This is the part that most Practice Fusion practice owners are skeptical about, and for good reason.
Many third-party tools promise digital forms but deliver a PDF that staff still have to open, read, and re-type. That is not a solution. That is the same problem with extra steps.
Curogram's write-back is different. When the patient submits the form, the data flows into structured fields in Practice Fusion. Demographics go to demographic fields. Medications go to the medication list.
Allergies go to the allergy section. Insurance information populates insurance fields. The chart is ready before the provider walks in.
A PDF attachment is searchable only if you open it. A structured field is searchable, auto-populates clinical forms, and feeds into billing and reporting.
The difference matters for every downstream task: prescription writing, insurance verification, care documentation, and follow-up scheduling.
|
Feature |
Paper + Manual Entry |
PDF Attachment |
Curogram Write-Back |
|
Patient completes before visit |
Rare |
Possible |
65-70% completion |
|
Staff re-entry required |
Yes (10-15 min) |
Yes (still re-typed) |
No |
|
Data in structured fields |
After re-entry |
No |
Yes, automatically |
|
Handwriting errors |
Common |
Common |
Eliminated |
|
HIPAA compliant storage |
Paper (risky) |
Depends |
Yes, encrypted |
Not every clinic needs the same form. A family medicine practice collects different information than a dermatology office or a pediatric clinic.
Curogram's form builder lets practices create intake forms that match their specialty and their workflow. Consent forms, screening questionnaires, and patient history sections are all customizable.
Forms are sent 24 to 48 hours before the appointment as part of the reminder sequence.
They arrive when patients are at home and have time to fill them out carefully, not when they are standing at the front desk trying to remember their insurance plan name.

Most practice owners think of paper intake as a minor operational hassle. The numbers tell a different story.
The cost of staying on paper shows up in staff hours, printed supplies, downstream billing errors, and slower patient flow every single day.
Manual data entry takes 10 to 15 minutes per patient. For a practice seeing 20 to 30 patients per day, that is 3 to 7 or more hours of staff time spent on transcription alone.
At $18 to $25 per hour for front desk staff, that works out to $1,000 to $3,000 or more per month in labor costs just for typing in what patients already wrote down.
That time is not idle time. It is time taken away from insurance verification, billing follow-ups, patient calls, and everything else that keeps a small clinic running. When staff are transcribing, they are not doing anything else.
|
Patients/Day |
Entry Time/Patient |
Daily Hours Lost |
Monthly Labor Cost (at $20/hr) |
|
20 |
10 min |
3.3 hrs |
~$1,320 |
|
25 |
12 min |
5.0 hrs |
~$2,000 |
|
30 |
15 min |
7.5 hrs |
~$3,000 |
These are conservative estimates. They do not include time spent hunting down illegible entries or correcting errors found during billing.
A 19-page intake packet per new patient adds up quickly. Paper, toner, printing, clipboards, and document storage are recurring expenses.
Add HIPAA-compliant shredding for disposed forms and the cost compounds further. These are not large single expenses, but they are entirely avoidable with digital forms.
Online patient forms eliminate these costs completely. There is nothing to print, nothing to store, and nothing to shred. The savings are modest per patient but meaningful at scale.
When patients arrive without pre-completed paperwork, check-in takes 15 to 20 minutes for new patients. That creates a bottleneck that ripples through the entire schedule.
The provider starts late. Exam rooms back up. Patients who arrived on time end up waiting longer because the patient before them was still filling out forms.
Pre-visit digital intake cuts check-in to under five minutes. For a practice seeing 25 patients per day, that recaptured time translates directly into better patient flow and fewer late-running appointments.
Based on our internal research, practices that switch to text-linked intake see check-in times drop by more than 60%.
Numbers are useful, but a real story makes the stakes concrete. Here is how one small Practice Fusion clinic made the switch from paper to digital intake and what happened next.
A three-provider family medicine practice in suburban Atlanta had been running on Practice Fusion for four years.
The office manager, Denise, oversaw a two-person front desk team that handled check-in, phone calls, and chart preparation. The practice saw 60 to 70 patients per day across three providers.
Every new patient received a 19-page intake packet at the door. Returning patients filled out updated forms for medication changes, insurance updates, and annual questionnaires. Front desk staff estimated they spent 4 to 5 hours per day on manual data entry into Practice Fusion.
Denise's team had attempted to use Practice Fusion's built-in Online Check-In feature. Setup was complicated, and only about 10% of patients completed it before arrival.
The rest showed up expecting the clipboard. The practice had also looked at Updox as an alternative, but the added cost layered on top of the Practice Fusion subscription was a dealbreaker.
The result was that both systems ran in parallel: some patients came in with digital forms, most did not, and staff had to manage both. It created more confusion than it solved.
Denise activated Curogram's Text-to-Chart Pipeline. Custom intake forms were built to match the existing paper packet: demographics, insurance, medical history, medications, allergies, and consent forms.
The forms were set to send via text 24 hours before each appointment. Staff learned the system in a single morning session.
Within four weeks, 65 to 70% of patients completed their intake forms before arrival. New patient check-in dropped from 20 minutes to under five.
Data entry hours were cut by more than half. Staff redirected that time toward insurance verification and billing follow-ups.
The improvement was not invisible to the clinical team. Providers opened charts that were already complete instead of seeing notes that said "pending intake."
Medications were spelled correctly. Insurance IDs were accurate. Phone numbers were validated. Transcription errors dropped noticeably in the first month.
Denise's summary was direct: "We stopped buying paper. We stopped printing packets. My staff stopped squinting at handwriting. The patients love it because they do it on their phone in two minutes. This should have been the default from day one."
Moving from paper to digital raises a fair question: is it actually more secure? The answer is yes, and by a wide margin.
A paper form sitting on a clipboard in a waiting room is far less protected than encrypted data moving through a HIPAA-compliant platform.
All data transmitted through Curogram is encrypted and HIPAA compliant. Curogram signs a Business Associate Agreement (BAA) with every practice before any patient data is exchanged.
This means Curogram operates as a covered business associate under HIPAA, with the same obligations and protections that apply to the clinical data in your chart.
Compare that to paper. A filled-out intake form can be left on a desk, seen by someone walking by, or misplaced during a busy morning.
There is no audit trail for paper. There is no access log. Digital intake, managed through a HIPAA-compliant platform, provides both.
The Business Associate Agreement defines how Curogram may use and safeguard patient data, what happens in the event of a breach, and the remedies available to the practice.
It is not optional. Every practice using Curogram for patient intake has a signed BAA on file before the first form goes out.
Practices are also required to use the platform in ways that stay HIPAA-compliant on their end, including not modifying default SMS templates to include protected health information and restricting platform access to authorized staff only.
Digital intake forms include e-signature capture for consent forms, HIPAA acknowledgments, and financial responsibility agreements.
Patients sign on their phone. Signed forms are stored securely and linked to the patient's record in Practice Fusion.
This replaces the chronic problem of missing paper consents. No more searching through a file cabinet for a form the patient swears they signed.
No more "did they initial this page?" questions. Every signed document is in the chart, accessible when needed.
Yes. Electronic signatures on medical consent forms are valid under the Electronic Signatures in Global and National Commerce Act (E-SIGN Act) and the Uniform Electronic Transactions Act (UETA).
Digital consent forms captured through a HIPAA-compliant platform meet the same legal standard as a wet signature on paper.
The additional benefit is that digital signatures are time-stamped, tied to the patient's identity, and stored with an audit trail. A paper signature has none of those attributes.

Switching to digital intake should show up in your numbers. Here are the key metrics that practice owners and office managers should track before and after activating the Text-to-Chart Pipeline.
This is the first metric to watch. Track the percentage of patients who complete their intake forms before they arrive.
A healthy target is 60 to 75% within the first month of launch. For context, portal-based completion rates at small Practice Fusion clinics often sit below 15%.
Text-linked forms perform better because patients do not need to log in or remember a password. They tap a link in a text message, which is something most people do dozens of times a day. That low barrier is what drives higher completion rates.
Curogram's dashboard shows which patients completed their forms and which did not before each appointment.
Practices can monitor this weekly and see the completion rate trend upward as patients become familiar with the new process.
Within 30 days, most clinics reach a stable completion rate well above what any portal-based system achieved.
Before switching, ask your front desk team to log the time they spend on manual chart entry for one week. This gives you a baseline.
After activating digital intake, repeat the measurement. The target is a reduction of 50% or more.
For a practice that was spending 4 to 5 hours per day on data entry, that means recovering 2 to 3 hours daily.
Based on our internal data, practices using Curogram's text-linked intake cut manual data entry hours by more than half within the first month.
The hours recovered from data entry do not disappear. They go back into the work that matters. Insurance verification. Billing follow-ups. Patient callbacks. Prior authorization requests
These are high-value tasks that get deferred when staff are tied up with transcription. Reducing data entry frees your team to do work that directly affects revenue and care quality.
Track average check-in time for new patients before and after the switch. With paper, new patient check-in typically runs 15 to 20 minutes.
With pre-completed digital intake, it drops to under five minutes.
Faster check-in has a compounding effect on the rest of the day. The provider stays closer to schedule. Rooms turn over faster.
Patients in the waiting room wait less. The entire day runs more smoothly when the front desk is not managing a paper-filling queue at 9 a.m.
|
Metric |
Before (Paper) |
After (Digital Intake) |
Target Improvement |
|
Pre-visit completion rate |
<15% |
60-75% |
4x increase |
|
New patient check-in time |
15-20 min |
<5 min |
60%+ reduction |
|
Daily data entry hours |
3-7 hrs |
1-2 hrs |
50%+ reduction |
|
Transcription error rate |
Common |
Near zero |
Significant drop |
Moving from the "clipboard era" to a digital-first workflow isn't just about following a trend—it’s about closing the security gaps and efficiency drains that paper intake creates.
As we’ve explored, the risks of untraceable audit trails and manual data entry aren’t just administrative headaches; they are direct threats to HIPAA compliance and your practice's bottom line.
The most effective way to eliminate these risks is to meet patients where they already are: on their smartphones.
By integrating Curogram with Practice Fusion, your practice can finally replace the physical stack of paper with a seamless, text-linked digital experience.
Unlike traditional "digital" solutions that merely generate a flat PDF for you to download and manually upload later, this integration focuses on structured data.
Modern healthcare requires modern tools. Your patients already manage their banking, travel, and shopping from their phones.
They expect (and appreciate) that same level of convenience from their healthcare provider. When you remove the friction of the waiting room clipboard, you aren't just improving their experience; you are giving your front-desk staff the gift of time.
Instead of hunting down missing signatures or squinting at illegible ink, your team can focus on what they do best: patient care.
Schedule a demo to watch a live text link go out, see the patient-side experience, and witness the data flow directly into Practice Fusion. It’s time to put the clipboard away for good.

💡 Practice Fusion front desk data entry is one of the biggest time drains in small clinics. When a patient fills out a paper form, and staff have...
💡 Practice Fusion patient intake forms powered by Curogram let patients fill out all check-in paperwork on their phone before they arrive. No app...

💡 Curogram delivers the eClinicalWorks patient digital form experience through text — with no app download, no clipboard, and no lobby wait....