
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
How to Strengthen Opus EHR Data Integrity with Digital Patient Intake
💡 Behavioral health facilities protect Opus EHR clinical data integrity through digital patient intake that replaces manual paper forms. ...

A patient calls your center at 9 a.m. Today is the day they decided to get help. They qualify for a bed. Then the paperwork starts.
Before anyone can assign that bed, they have to finish a thick stack of forms — consent documents, insurance details, clinical screenings. Each page is one more small reason to pause, and pauses are exactly what you cannot afford here.
In addiction treatment, a pause is dangerous. The patient is ready. Your team is ready. The forms are not.
One prospect put it plainly: "We have 19 pages of paper forms per patient." Staff print them, hand or mail them, wait, then key every single answer into the system by hand.
That delay is not just annoying. It sits right in the window between "yes" and "admitted," the window where people reconsider and walk away. Curogram's Opus integration was built to close it.
Here is the shift. Digital intake for SUD admissions on Opus moves that whole stack to the patient's phone. They tap a secure link, fill out consent, upload an insurance card, and complete screening before they walk in.
The answers flow straight into the Opus record.
No re-typing. No lost pages. No second round of data entry by your front desk team.
This article walks through what that change looks like in practice. You will see what paper intake really costs you, why your current tools cannot fix it, and how a simple text link turns a half-day bottleneck into a 30-minute task.
We will keep it concrete. Real workflow steps, plain numbers, and honest trade-offs. By the end, you will know exactly how same-day admissions speed up when intake starts the moment a patient qualifies instead of the moment they arrive.
So let's begin where the delay always begins: the paperwork.
Same-day admission is the standard in SUD treatment for a reason. A patient calls, qualifies, and needs intake done before a bed opens to them. The clock between that "yes" and the actual admission is clinically fragile.
Delay that moment and the risk goes up. A longer wait gives a patient in crisis more time to reconsider, leave, or relapse. So the real enemy here is time, not paper itself.
But paper is what eats the time. The workflow looks like this:
Print the forms, hand or mail them, wait for the patient to finish, manually type every answer into Opus, verify insurance by phone, then file the physical copies.
For a center handling 5–10 admissions a day, that adds up fast. Each step is small. Together they consume hours of staff time and push bed assignment later into the day.
Here is a simple way to see the cost. Say staff spend about 45 minutes per patient just handling forms and re-entry, and you admit 8 patients a day.
| Daily admissions | Minutes of form handling each | Staff hours lost per day | Staff hours per week |
|---|---|---|---|
| 8 | 45 | 6 | 30 |
That is roughly 30 hours a week your team spends moving paper instead of supporting patients. This means almost one full-time role disappears into a task software could handle.
The money leaks too. Paper billing alone runs $800 to $1,000 per month at practices that see only a 20% conversion rate on mailed statements. For your team, that is a recurring cost with very little to show for it.
And Opus is not the problem. Opus manages the clinical record beautifully once a patient is admitted. It was simply never designed to run the pre-admission chase of collecting documents and chasing signatures.
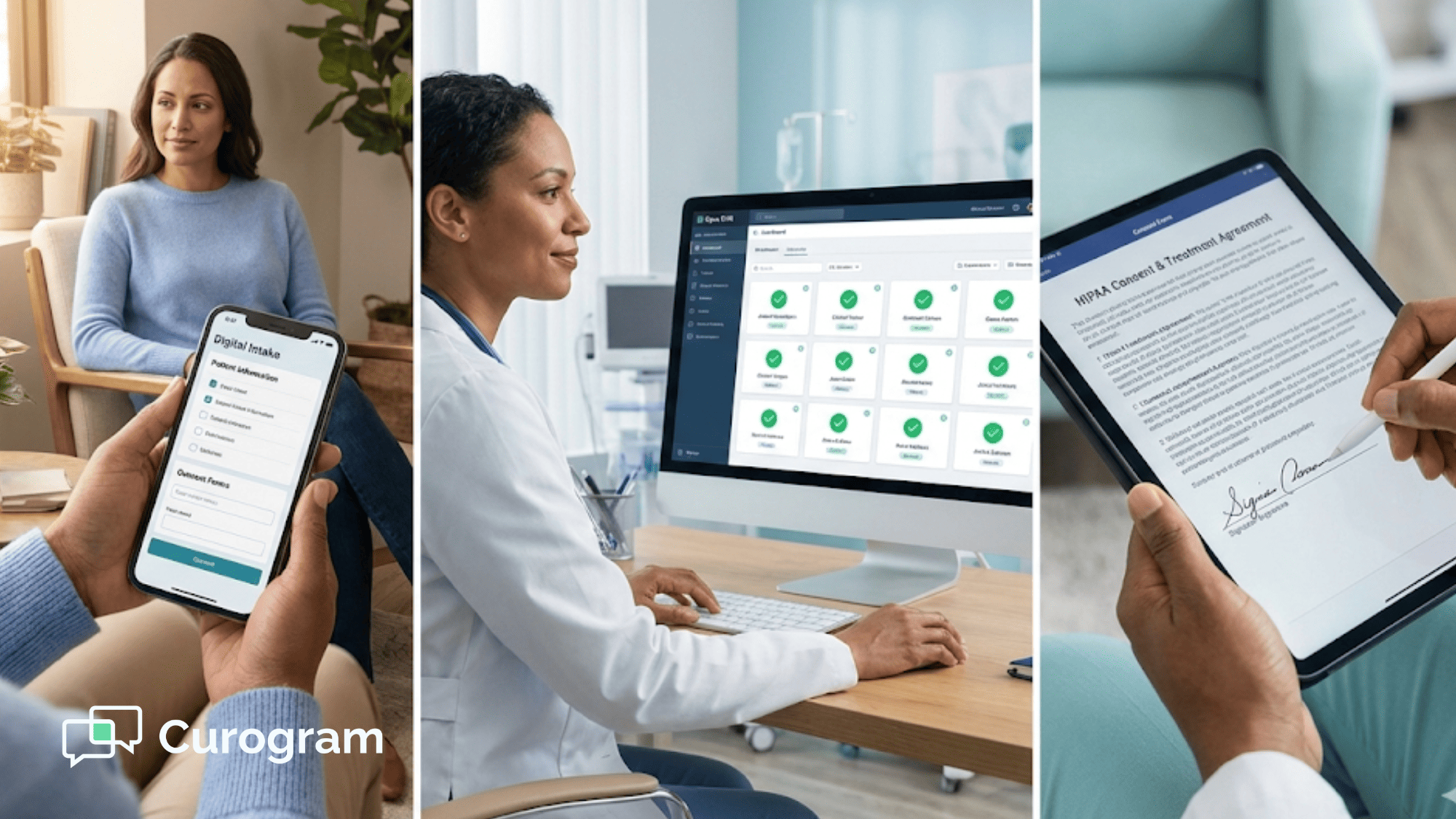
The easiest way to understand digital intake is to look at what it removes. Each manual step gets replaced by something faster that the patient can do themselves.
| Old paper step | New digital step |
|---|---|
| Printed consent forms | Consent signed by text link |
| Insurance verified by phone | Insurance card uploaded as a photo |
| In-person clinical screening | PHQ-9, GAD-7, and ASAM completed on the phone before arrival |
| Manual data entry into Opus | Responses sync straight to the Opus record |
The core change is about timing, not just format. Intake now starts the moment a patient qualifies, not the moment they walk through your door.
For same-day SUD admissions, that single shift compresses the timeline from hours to minutes. The forms are often done before the patient even leaves home.
Then there is the data itself. Completed responses sync into the Opus patient record through Curogram's Direct DB integration. No manual re-entry, no duplicate records, no paperwork lost between the fax machine and the chart.
The workflow is short enough to learn in one sitting.

Here is the full path from phone call to ready-for-admission:
That is the whole loop. Your coordinator sends a link, the patient taps it, and the chart fills itself.
Curogram's forms are fully customizable. A residential intake is not the same as an IOP intake, and neither matches a standard outpatient assessment, so you build each one to fit the program.
For centers serving diverse communities, forms can be set up in multiple languages. The patient gets the right document in the right words, with no extra lift from your staff.
All form data is transmitted and stored in HIPAA-compliant infrastructure, backed by a signed BAA. For SUD centers operating under 42 CFR Part 2, the form content can be configured to match Part 2 confidentiality rules.
The integration itself is the part most platforms cannot copy. Curogram connects to Opus through its patented Direct DB method, the only available pathway, since Opus does not offer a public API.
No other intake tool can push form data directly into an Opus patient record.
You may already be weighing a bigger name. It is worth reading Curogram vs Phreesia before you commit.
Phreesia is the enterprise intake standard, but it leans on multi-month rollouts, tablets and kiosks, and integrations Opus simply cannot support. Curogram is SMS-first, deploys in 2–4 weeks, and works with Opus out of the box.

The headline win is speed at the bed.
Same-day admission shifts from
"call in the morning, paperwork on arrival, admitted by afternoon" to
"call in the morning, forms done by phone within the hour, admitted on arrival."
The gains stack from there. Your intake coordinators move from data entry to clinical triage and patient support, which is the work that actually needs a human. Digital forms erase handwriting problems and the transcription mistakes that creep in by hand.
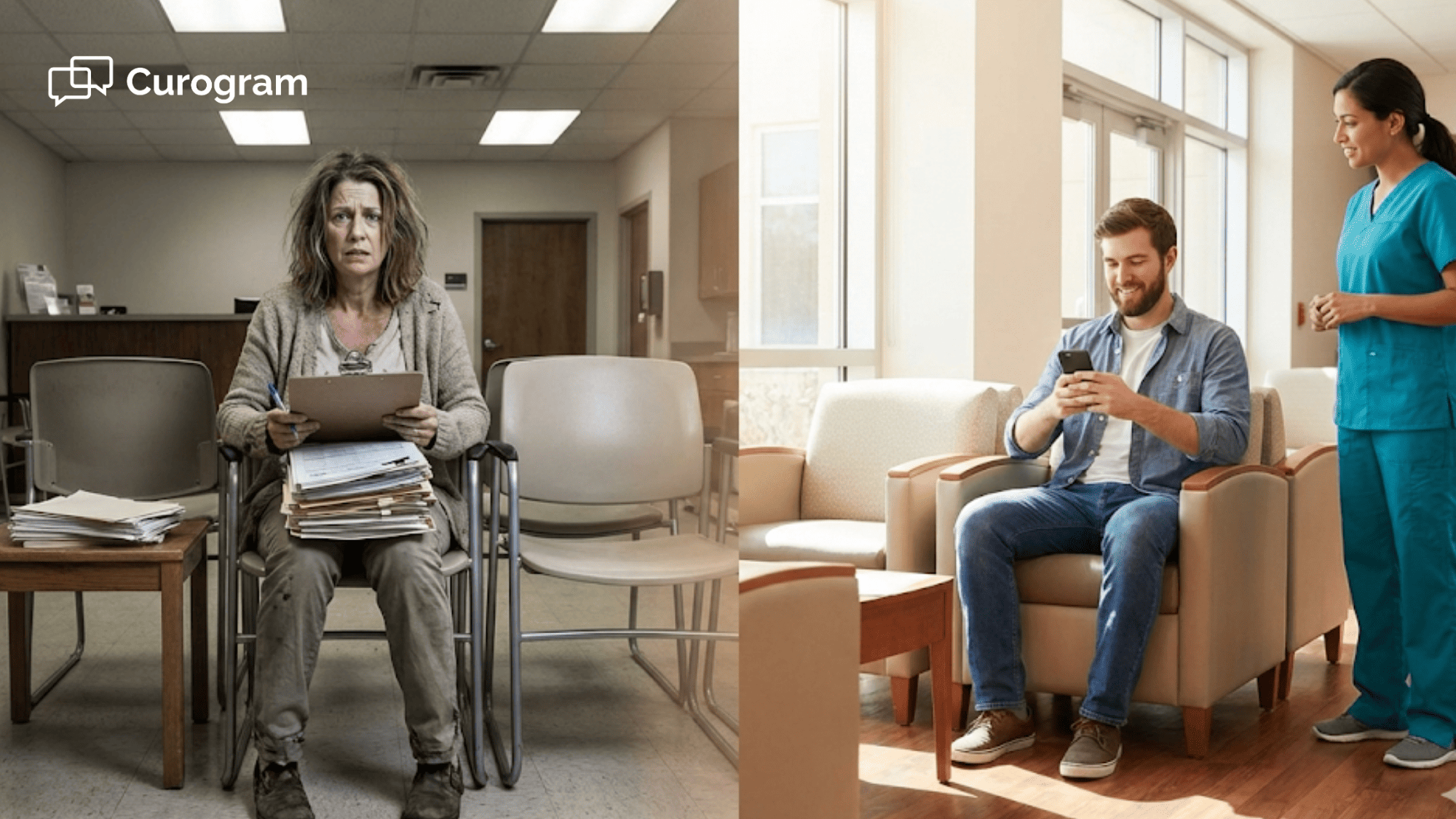
And a person who has just decided to enter treatment no longer hits a 19-page paper wall at their most vulnerable moment.
Each of those rolls into the same place:
Protected revenue. Every hour of intake delay is an hour the patient might reconsider, so compressing that window guards both the clinical outcome and the admission.
Think of it this way. If faster intake helps you hold onto even one patient a week who might otherwise have walked, that is roughly 50 additional admissions a year.
For your team, that is real census and real revenue recovered from a problem you used to accept as normal.
Getting started is lighter than most teams expect. Setup runs about 2–4 weeks from kickoff to live.
In that time, Curogram's implementation team handles the heavy parts for you:
There is no IT department required. No hardware to buy. No app for patients to download — just a text link they already know how to open.
If your center runs same-day SUD admissions and still moves paper to do it, this is the gap worth closing first. You can also see how Curogram serves behavioral health clinics across the rest of your workflow.
Here is the truth at the heart of SUD admissions. The hardest part already happened before the patient called you. They decided to get help.
Everything after that decision is yours to protect. And right now, for many centers, a stack of paper forms stands between a ready patient and an open bed.
That gap is where people slip away. Not because they stopped wanting treatment, but because the process gave them too many minutes to think, wait, and reconsider. The delay is quiet, but it is costly.
Digital intake for SUD admissions on Opus closes that gap by design. The forms move to the patient's phone, the answers flow straight into the Opus record, and intake starts the second a patient qualifies instead of the second they arrive.
The numbers behind it are simple to picture. Hours of staff form handling drop to minutes per patient. The $800 to $1,000 a month tied up in paper billing starts to shrink. And the same-day window that decides so many outcomes gets shorter, safer, and far easier to protect.
You also get there without the usual enterprise headache. No multi-month rollout, no tablets, no public API workaround. Just a text link, a 2–4 week setup, and a direct line into the Opus patient record that no other platform can match.
Most of all, you give patients a softer landing at their hardest moment, right when it matters in their recovery. A link, not a clipboard. A welcome, not a wait.
If you run same-day admissions on Opus, this is the friction worth removing first. See exactly how it fits your programs and your front desk in a short, focused walkthrough.
Book a Demo today and watch digital intake turn your admissions bottleneck into your fastest step.
💡 Behavioral health facilities protect Opus EHR clinical data integrity through digital patient intake that replaces manual paper forms. ...
💡 Digital patient intake for Opus EHR helps addiction treatment and behavioral health clinics speed up admissions and reduce paperwork. Patients...

💡 Digital intake forms built for Netsmart behavioral health integration replace paper packets with secure, mobile forms texted to consumers before...