
 Jo Galvez
Jo Galvez
CollaborateMD Digital Intake That Writes Back
💡CollaborateMD digital intake forms text link write-back replace 19 pages of paper, plus the manual re-typing behind them. Pawortients tap a secure...

Your front desk already holds every piece of intake data the patient just gave you. The patient typed it, signed it, and handed the packet back across the counter.
Then a staff member keys that same data into CollaborateMD by hand, one field at a time. That second step is quietly where most of the trouble begins.
We call this pattern the double-touch, and it hides in plain sight every single day. The patient fills out the form once, carefully, with all the right details.
Your staff then fills out the very same form again, this time inside the chart. Nothing new gets created, yet the odds of a costly error quietly double.
CollaborateMD does offer its own intake forms, so this is not a knock on the system. The catch is that the data often lands as paper or a flat file instead.
So the front desk still types names, dates, and long policy numbers by hand. Each keystroke becomes one more chance to mistype a digit that later bounces a claim.
That hidden cost is bigger than it looks at first glance. A misspelled name or a wrong birth date can quietly turn into a denial weeks later.
Then someone has to rework it, call the payer, and re-submit the whole claim. The hours you lose to re-typing come back again as hours lost to rejections.
There is a cleaner path, and it does not add a single new task for staff. When intake fills itself into the chart, the double-touch simply ends on its own.
This article shows how secure text-link forms write completed answers back to CollaborateMD. You will see how to reduce manual intake data entry errors without any extra work.
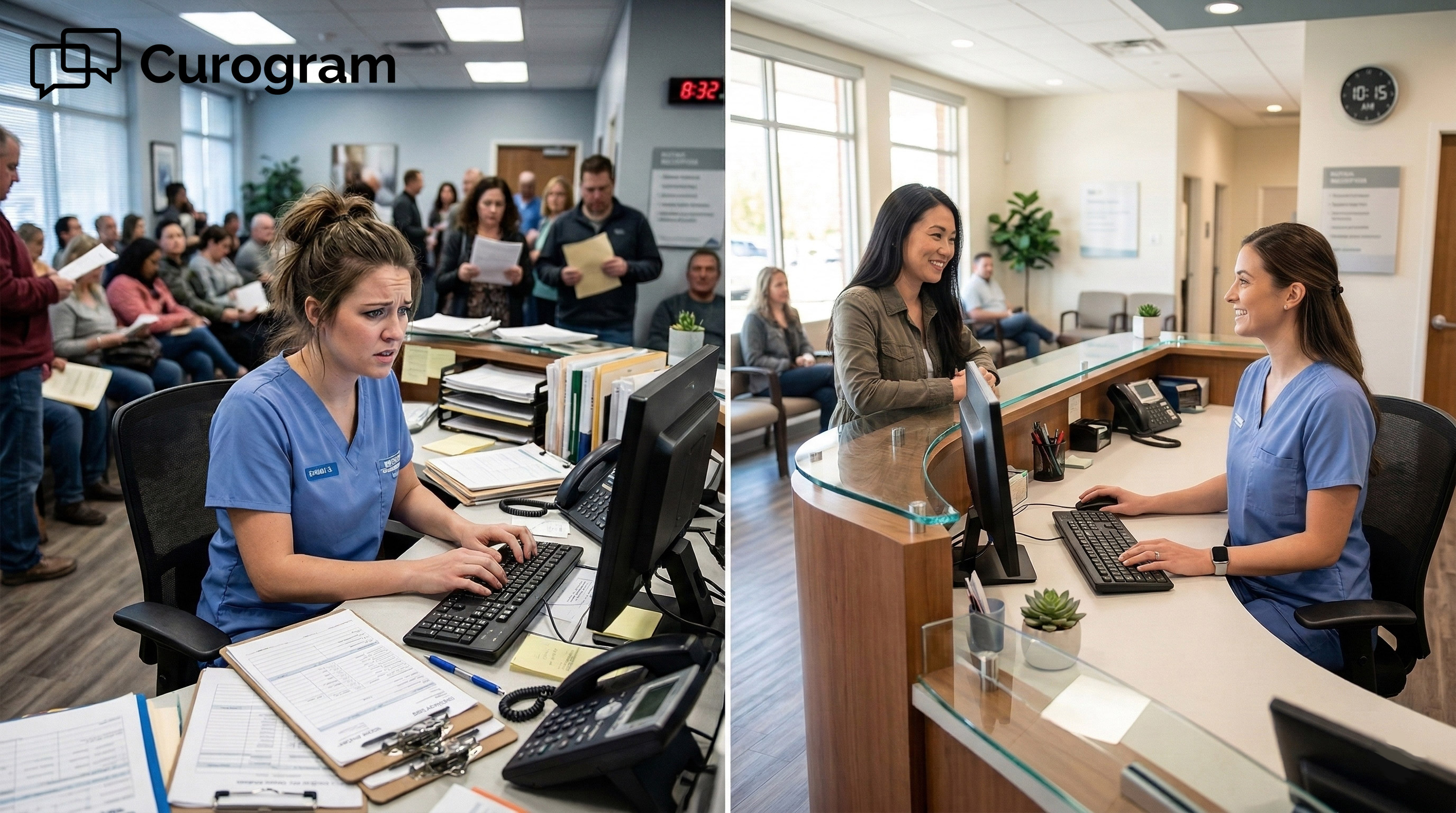
The double-touch is a quiet drain on both your staff and your revenue. It hides inside a daily routine that looks completely normal from the outside.
Let us break down exactly where it starts and what it truly costs you.
The forms themselves are real, and they work as intended. The problem is that the data arrives in the wrong shape for the chart.
CollaborateMD gives your practice a set of usable intake forms out of the box. Yet the answers often come back to you as paper or a flat file.
That means no clean, mapped fields flow straight into the structured chart. So a real person has to read each answer and type it in again.
This is true across primary-care, multi-specialty, and lab or diagnostic settings alike. The intake tool captures data, but it does not post that data for you. The gap between capture and chart is exactly where manual work sneaks back in.
The routine looks almost identical from one patient to the next. Print the packet, then start scanning paper forms into the CollaborateMD workflow.
Re-type every answer, file the paper copy, and move on to the next person. None of it creates anything the patient did not already hand you.
Each loop feels small, so it rarely shows up on anyone's report. Multiply that small loop by every visit, every day, across every provider. Suddenly, a huge share of front-desk time goes to pure transcription.
Re-typing is never truly free, even when it feels like part of the job. The bill shows up later, quietly, inside your billing and rejection queue.
HFMA reports that most denials come from provider-side process issues, including inaccurate patient information.
One wrong digit in a long policy number is all it takes. A single flipped birth date can do the very same damage.
These small intake errors cause claim denials to pile up faster than teams expect. Every re-typed field is really a denial quietly waiting to happen.
The denial does not appear at check-in, so no one links it to intake. It surfaces days later as a rejection that someone else now has to fix. By then the original typo is buried, and the rework clock is already running.
A billing company runs this exact process for many client practices at once. So the same risk stacks up across every single practice they serve.
Hours spent on data entry are hours not spent working the rejection queue. The math only gets worse with each new client the company adds.
One messy intake source can quietly infect dozens of downstream claims. Clean data at the front end is the cheapest fix available to them.

Now for the fix, and it is refreshingly simple in practice. Curogram quietly takes the keyboard out of the intake process altogether. The data fills itself into CollaborateMD, so that second touch never happens.
The patient still does the real work, but they only do it once. After that single step, the chart updates itself with no help from staff.
Curogram sends a secure form via 2-way HIPAA-compliant texting, straight to the patient's phone. They enter demographics, insurance, HPI, and ROS details in just a few quick taps.
The answers come back to you fully structured and ready to post. There is no packet to print and no stack of paper to chase down.
Because the form lives on the phone, patients can finish it before they ever arrive. That pairs neatly with appointment reminders, the pre-visit nudge that gets forms done early. By check-in, the hard part of intake is already complete and clean.
Completed fields write back into CollaborateMD through a direct HL7 or API link. The record updates on its own, with no scanning and no re-keying at all.
Forms built this way eliminate double data entry in CollaborateMD intake for good. Clean data lands exactly where the billing team needs it, the very first time.
Nothing sits in a queue waiting for a staff member to transcribe it. The moment the patient submits, the structured chart reflects their answers.
This is not a heavy IT project that eats your calendar for weeks. It fits neatly into the way your team already works today.
The CollaborateMD connection is already built, so there is nothing to wire up. Staff simply send a text link and then watch the chart fill in.
Training takes under 10 minutes because there is no new data-entry step to learn. This front desk manual data entry reduction shows up on the very first day.
There is no long onboarding and no thick manual for the team to study. People who can send a text message can already run the whole workflow.
Forms scale across all of your client practices from one shared dashboard. A billing company adds clean intake with no per-client setup project at all.
Automated intake write-back gives the billing team far fewer data-driven denials to chase. For RCM, clean intake data is the foundation everything else quietly stands on.
One consistent intake source means one consistent standard for every practice served. That standard is what turns messy data into a reliable revenue engine.
So what actually changes the moment intake begins to self-file? The extra step simply disappears from your team's daily list. Your staff stops transcribing and starts working on what truly moves revenue.
|
Step |
Double-Touch (Before) |
Zero-Touch (With Curogram) |
|---|---|---|
|
Patient fills form |
On a paper packet |
On their phone |
|
Data entry |
Staff re-type by hand |
Write-back posts it |
|
Error risk |
High, every field |
Low, no re-keying |
|
Intake-driven denials |
Common |
Rare |
|
Setup time |
Ongoing rework |
Under 10 minutes |
Two things go away for good once write-back is running. Neither one was ever actually helping your practice or your patients.
The 19-page paper packet stops existing the day text-link intake goes live. So does the filing drawer that used to hold every printed copy. Patients tap through a short, focused form on their phone instead.
A shorter form is also a form patients are far more likely to finish. More completed forms means more clean, ready data flowing into every chart.
The re-keying step is the real prize hiding inside this whole shift. Once write-back runs, nobody ever types the same data into the chart twice.
That removes the exact spot where most intake errors are quietly born. Fewer bad fields at the source means fewer denials waiting down the line.
You are not just catching errors faster with this approach. You are removing the step that created those errors in the first place.
Time and focus both come back to the front desk almost immediately. Both had been stuck in the wrong place for far too long.
Call the shift exactly what it is: from data entry to patient care. Staff stop transcribing forms and start helping the people in front of them.
The whole desk feels calmer because the endless busywork is finally gone. Patients notice the smoother, faster check-in the moment they walk in.
A calmer front desk also makes fewer rushed mistakes on the phones. The good effects ripple outward across the entire patient visit.
Fewer of your denials now trace back to bad or mistyped intake. The hours once lost to re-typing quietly return to the whole team.
That reclaimed time can go to the rejection queue or to patients directly. Either way, the time now works for your revenue instead of against it.
Clean claims are submitted faster, so payment arrives sooner and more reliably. That steadier cash flow is the quiet reward for ending the double-touch.

Here is the whole idea distilled down into a single line. Write-back intake ends the double-touch for good, quietly and completely.
Your staff stop creating the very errors that re-typing always introduces. They also stop reworking those same errors again weeks later.
The double-touch always looked like normal, necessary work to everyone involved. Someone had to type the packet into the chart, so someone always did.
But typing in the data the patient already gave you never added any real value. It only added fresh risk to every claim that followed.
It helps to think about the two tools by their actual jobs. CollaborateMD is your chart of record, built to hold and protect the data.
Curogram handles the patient's one-time typing and delivers it in clean. Together, intake finally stops generating denials instead of quietly causing them.
So it is worth changing how you measure intake success altogether. Stop counting how many forms your team scanned last month.
Start counting how many claims are submitted cleanly on the very first try. That single number is the one that actually pays the bills.
Picture the last denial your team had to rework from scratch. Odds are good that it started with a single mistyped field. Now, picture that field never getting mistyped in the first place. That is the quiet promise of self-filing intake.
This is where Curogram helps CollaborateMD practices reduce manual intake data entry errors. Clean, structured data now flows straight into the chart on its own. The billing team inherits far fewer data-driven denials to chase each week. The front desk earns back its lost hours at the very same time.
The payoff quietly spreads across your whole pre-visit flow. Forms arrive already done, so check-in moves faster for everyone.
The desk feels calmer, and your patients can feel that shift too. Everyone ends up spending less time on paper and more time on care.
Rural clinics, community hospitals, and busy billing companies all feel the same drain. Every one of them keys in data that the patient already supplied.
Ending that habit frees people to focus on care and clean claims. The tool does the typing, so your team does not have to.
None of this asks your team to learn a hard new system. The heavy lifting happens automatically, behind the scenes, on every visit. Fix the source once, and the benefits repeat with every single patient.
Ready to see it work on a real chart of your own? Complete your revenue cycle and schedule a demo today.

💡CollaborateMD digital intake forms text link write-back replace 19 pages of paper, plus the manual re-typing behind them. Pawortients tap a secure...
💡 eClinicalWorks secure online forms with structured data intake for enterprise networks replace clipboard-based check-in with text-delivered...

💡 Practice Fusion front desk data entry is one of the biggest time drains in small clinics. When a patient fills out a paper form, and staff have...