
.jpg) Mira Gwehn Revilla
Mira Gwehn Revilla
Automate Sigmund AURA Client Intake Forms for Behavioral Health
💡 Sigmund AURA client intake forms automation for behavioral health works best with a self-service form tool layered on your EHR. Curogram lets...

Your clinical director wants a new screening added to the intake packet. It sounds like a quick, five-minute task. But in Sigmund AURA, that small change becomes a support ticket. Then you wait.
This is the daily reality for many behavioral health intake teams. Sigmund AURA handles clinical records and treatment notes well. Yet its embedded forms are not built for fast edits by staff. Adding one field or updating consent language often means waiting on the vendor.
So the form sits in a queue while the program launches. Staff print the new screening on paper to fill the gap. Now intake runs half digital and half paper. Data entry doubles, and clients notice the messy mix.
There is a better way to run this. A Sigmund AURA intake workflow setup with staff self-service forms gives control back to your team.
Instead of filing tickets, your intake coordinator builds and edits forms directly. The clinical chart still lives in Sigmund, and the intake layer simply moves faster.
This is where a Sigmund AURA form builder alternative setup helps. Curogram works as a separate form layer beside your EHR. It needs no API access and no changes to Sigmund itself. Your team makes packets, sends them by text, and reviews answers on one dashboard.
The payoff is real ownership of your behavioral health intake workflow configuration. New screenings, fresh consent forms, and updated insurance fields go live in minutes. The people who know intake best finally control it. That ownership changes how your whole intake day runs.
This guide shows how that setup works from start to finish. You will learn how to build packets, send them, and stay compliant. By the end, you can stop the vendor wait for good. Your intake team gets the control it has always needed.
Sigmund AURA does offer digital intake. But "digital" comes with a catch. Based on user reports, Sigmund staff must add each form item by hand. The forms are embedded, so quick edits stay out of your control.
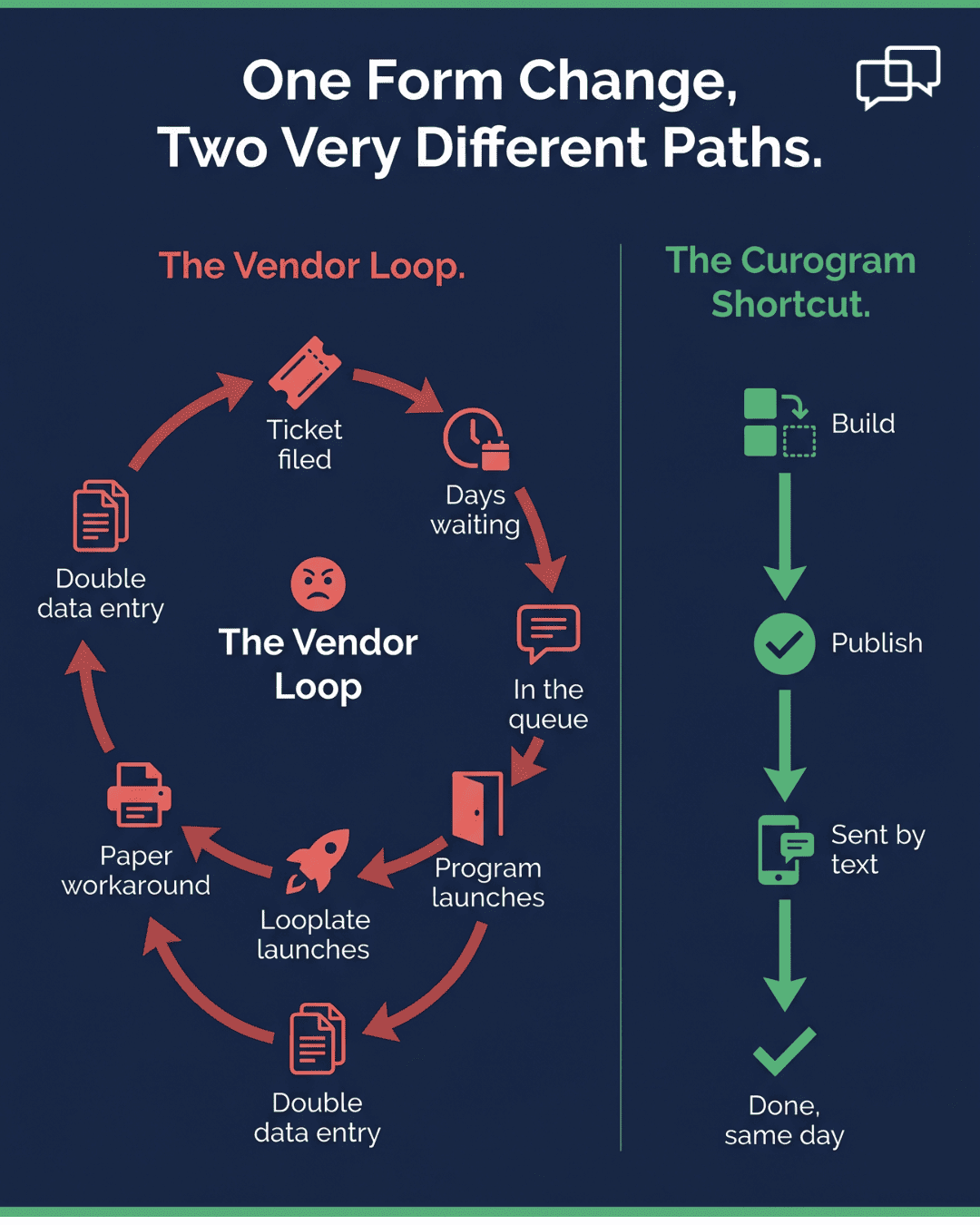
This creates what we call the vendor dependency loop. Your intake coordinator cannot add a field, change a consent form, or drop in a new screening alone. Each change starts with a support ticket. Then the waiting begins.
|
Here is how it plays out in real life: Your clinical director adds the CAGE-AID screening for a new SUD program starting next month. The intake coordinator files a ticket with Sigmund. Days pass with no fix. A follow-up email gets one reply: the change is in the queue. The program launches anyway. The CAGE-AID is still missing from the digital packet. Staff print it on paper to cope. |
Now intake runs half digital and half paper, and the data entry load doubles. This kind of Sigmund embedded forms workaround feels normal after a while. But it quietly drains your team every single week.
Each vendor-led change costs you in three ways. The table below breaks them down.
|
Hidden cost |
What it looks like |
Who feels it |
|
Time |
Days or weeks waiting in the support queue |
Intake coordinator, clinical director |
|
Labor |
Staff print, scan, and re-key paper forms |
Front desk and intake staff |
|
Accuracy |
Handwritten forms cause typos in the chart |
Clinicians and billing |
Let's put rough numbers to the labor cost. These are example figures, not hard data. Say your program adds 10 to 15 new clients each week. Each paper form takes about 15 to 20 minutes to re-enter.
That is roughly 3 to 5 hours of staff time every week. Over a year, the math adds up fast. At common front-desk pay rates, the re-entry work could cost $15,000 to $25,000. You pay staff to retype data the client already gave you on paper.
The deeper problem is the hybrid system no one chose. Some forms live in Sigmund's embedded tool. Others are printed and scanned. The newest ones exist only as PDFs emailed to clients who may never finish them.
The intake coordinator says it best.
I spend more time managing the workarounds than I would building the forms myself."
That is the loop. And it repeats every time a form needs to change.
For behavioral health teams, forms change all the time. New screening tools replace older ones. Agencies update consent rules.
Payers shift their verification fields, and new programs launch with their own needs. A system that turns every edit into a vendor task simply cannot keep up.
Curogram fixes the loop with one simple shift. It puts form creation, editing, and delivery fully in your intake coordinator's hands. Changes that took days through Sigmund now happen in minutes.
The heart of this is the drag-and-drop form builder. It ships with templates for common behavioral health screening tools. You get PHQ-9, GAD-7, AUDIT-C, and CAGE-AID ready to use. You also get consent forms with 42 CFR Part 2 language for SUD programs.
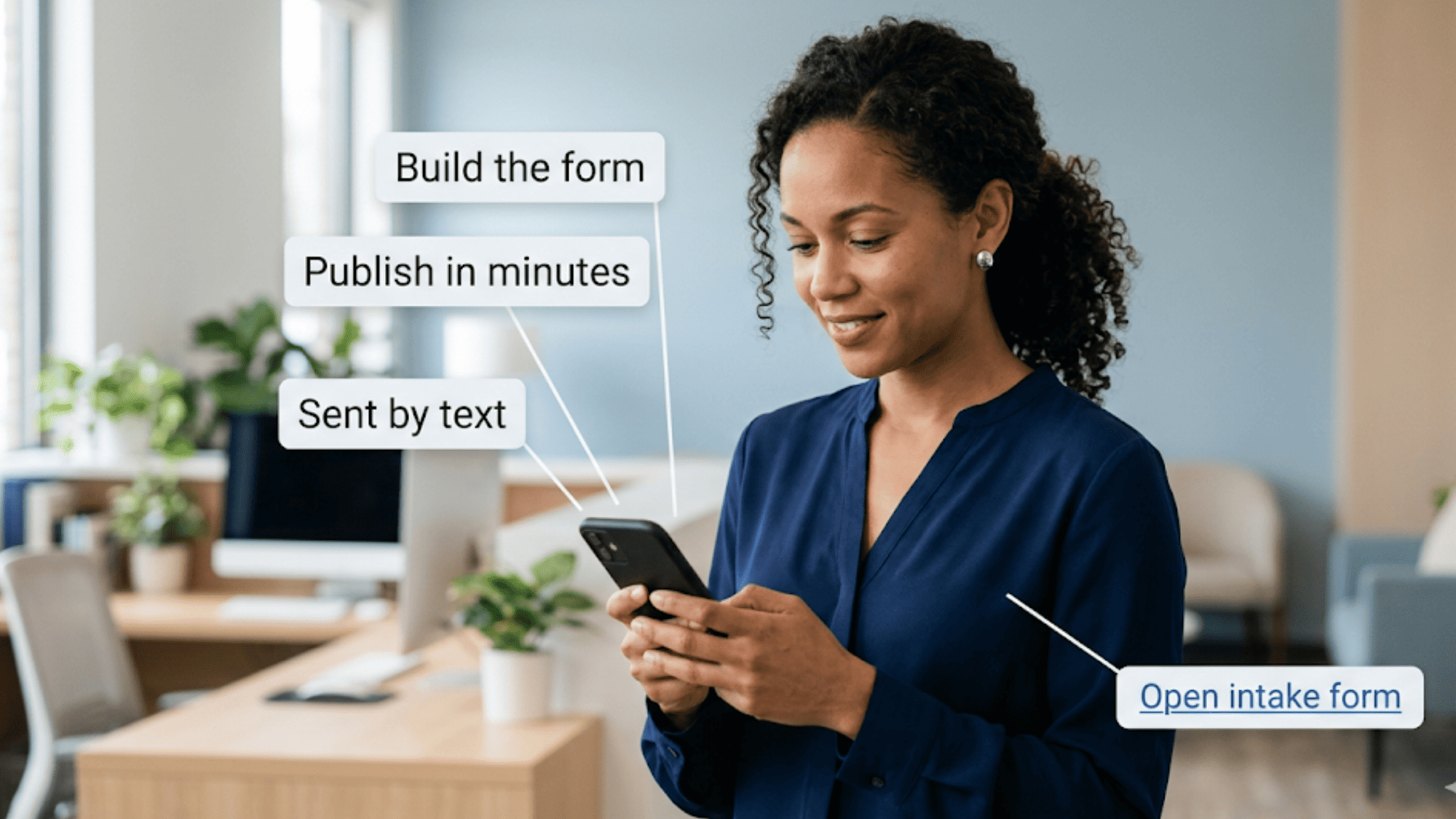
Building a packet is straightforward. Here is the basic flow your team follows:
That is the whole process. You get self-service digital forms EHR integration without touching Sigmund's core setup. The two systems stay separate, so nothing breaks on the clinical side.
This matters for the setup itself. Implementation requires no Sigmund API access. Curogram runs as an independent form delivery and collection layer. Forms go out by text, clients fill them on mobile, and answers land in a clean dashboard for clinical review.
The learning curve is short, too. Curogram form builder onboarding for Sigmund teams takes one quick session. Most intake coordinators build and send their first form within 15 minutes. There is no coding and no IT ticket to wait on.
Because intake here never sits still. New evidence-based screenings replace older versions. Regulators update consent requirements. Payer contracts change the fields you must collect, and new programs launch with special needs.
A form system that staff control keeps pace with all of it. When the clinical program changes, the intake packet changes the same day. There is no vendor bottleneck between the idea and the live form. Your team moves as fast as your clinic does.
Think of it as a trade you control. With Sigmund's embedded forms, speed depends on the vendor's queue. With Curogram, speed depends on you. The work shifts from "file a ticket and hope" to "build it and send it."
This is the core promise of a true self-service setup. Your forms are no longer frozen between updates. They grow, shrink, and adjust as your programs do. And every change stays compliant from the first click to the last.
That control adds up to real time back in your team's day. When forms stop waiting on a queue, your coordinators spend their hours on clients instead of workarounds. To see what those reclaimed hours could be worth, use our staff efficiency ROI calculator and map the savings to your own intake volume.
The biggest win is simple. Your team reclaims hours each week and stops chasing the vendor. Let's look at what that change really delivers, in numbers and in daily life.
Start with the time savings:
Using the same example math from earlier, each paper re-entry takes 15 to 20 minutes. With self-service digital forms, the client types the data once, and it flows straight to your dashboard.
For a program adding 10 to 15 clients a week, that frees roughly 3 to 5 hours of staff time. Those hours go back to patient care instead of retyping.
Now look at the ticket count. It drops to zero. There are no support requests to update a form, swap a screening, or fix consent wording. Your intake coordinator handles all of it in the builder. The chart below shows the shift clearly.
|
What changes |
Vendor-controlled forms (before) |
Staff-controlled intake (after) |
|
Add a new screening |
File a ticket, wait days or weeks |
Drag it in, publish in minutes |
|
Update consent language |
Email the vendor, follow up twice |
Edit and republish the same day |
|
Launch a new program packet |
Half-digital, half-paper stopgap |
Full digital packet ready at launch |
|
Re-entry of paper forms |
3–5 hours of staff time weekly* |
Near zero; clients enter data once |
|
Form update tickets |
Several per month |
Zero |
*Illustrative estimate based on 10–15 new clients per week.
This is the move from "vendor-controlled forms" to "staff-controlled intake." Form updates, new screening tools, and consent changes get managed by the people who know intake best.
That is intake coordinator form management for behavioral health, finally done on your team's terms. The vendor queue stops being the gatekeeper.
Here is what a normal day looks like after the switch. The clinical director adds a new trauma screening to the IOP intake protocol at 9 a.m.
The intake coordinator opens the builder and pulls the screening fields from a template. She previews the mobile layout, checks the flow, and hits publish, all before lunch.
That afternoon, the next new IOP client gets the updated packet by text. They tap the link, fill it out on their phone, and submit. The answers appear in the dashboard, ready for clinical review. No ticket. No wait. No paper backup.
Multiply that across a busy week and the impact grows. A SUD program might update consent for a new grant requirement. A PHP track might add an insurance field for a new payer. Each change goes live in minutes, not weeks. Your packets stay current without a single vendor email.
The data backs up the broader payoff, too. When practices automate intake and engagement, the numbers move.
Based on our internal data, Atlas Medical Center cut no-shows from 14.2% to 4.91% in just three months. Their intake automation was one part of that larger engagement overhaul. That result ran about 3X better than the industry average.
Why Curogram Gives Your Intake Team Control Without an EHR Overhaul
Curogram is a patient engagement platform built for practices that need speed and control. It works beside your EHR, not on top of it. That design choice is the whole point. You keep Sigmund AURA for clinical records and add Curogram for the intake layer that feeds them.
Because the two stay separate, you skip the risky overhaul. There is no API project, no data migration, and no downtime for your clinical system. Your intake coordinator simply logs into Curogram and starts building forms. Sigmund keeps doing what it does best.
The value shows up fast across the practice. Curogram's self-service builder removes the vendor queue for every form change. Its text-based delivery meets clients where they already are, on their phones. And its dashboard keeps every completed packet organized for clinical review.
The broader results speak for themselves. Based on our internal data, one practice cut no-shows from 14.2% to 4.91% in three months. More than 75% of Curogram clients reach strong appointment confirmation rates. Many also see up to 50% fewer inbound phone calls and a 30%+ gain in staff productivity.
Compliance is built in from setup through daily use. Curogram is HIPAA, SOC 2 Type II, and 42 CFR Part 2 compliant. That matters most for SUD and behavioral health programs with strict consent rules. Your team can move fast and stay safe at the same time.
The takeaway is simple. Curogram hands form control to your staff without forcing a system change. You get speed, accuracy, and ownership, while Sigmund holds the clinical chart. It is the missing intake layer, ready in a single short session.
Sigmund AURA's embedded forms keep your behavioral health intake locked behind ongoing vendor dependency. Every small update has to sit and wait in a support queue your team cannot control.
Days pass, the program launches, and printed paper steps in to fill the gaps. Curogram's self-service form builder hands that everyday work straight back to the staff who own it.
With it, your intake coordinator can create, edit, and send forms on the very same day. There are no tickets to file, no API to wire up, and no vendor delays to absorb. The change you need first thing this morning can be live for clients by lunch. That speed is what real control over your intake workflow looks like.
It helps to picture Sigmund AURA and Curogram working together as one clear team. Sigmund holds your clinical records, treatment notes, and the long-term history of each client.
Curogram fills the intake layer that feeds clean, accurate data into those records. One tool stores the chart, and the other quietly does the work to complete it.
Better still, Curogram completes that chart fully on your team's terms. This matters most when new programs grow fast or when compliance rules suddenly shift.
Fresh screenings and updated consent forms can keep pace with the clinic without delay. Your intake team adapts in minutes instead of losing weeks to a slow queue.
Bring your messiest intake packet to a quick demo call and we'll show you how to turn it into a same-day, text-ready form in minutes.

💡 Sigmund AURA client intake forms automation for behavioral health works best with a self-service form tool layered on your EHR. Curogram lets...
💡 Eliminating data re-entry in Elation Health practices means capturing patient details once — and never typing them again. Curogram's digital...

💡 Digital behavioral health intake forms Opus EHR admission workflow tools fix a known gap. Opus EHR offers digital intake forms, but the data does...