
 Jo Galvez
Jo Galvez
SMS Intake Forms for Opus EHR | Save 60 Min Per Admission
💡 Opus EHR handles clinical notes well, but its intake forms have a gap. Patient data does not auto-populate into the chart. Staff must copy and...

It's 9 AM on a Monday. The intake coordinator has three residential admissions, two IOP starts, and a referring hospital waiting on a bed confirmation.
Each new patient has already filled out digital forms online. Yet the coordinator still spends an hour per patient retyping every field into Opus EHR.
The forms are digital. The data is digital. But the two systems do not talk to each other. So staff become human copy-paste machines for 19+ pages of consent, history, and insurance details. That is the problem.
Opus EHR is a strong clinical platform for behavioral health and SUD treatment programs. Yet a documented gap exists: intake form data does not flow into the patient record.
Online patient forms behavioral health SUD teams collect end up sitting in PDFs, waiting on a human to type them in.
This blog walks through how digital behavioral health intake forms Opus EHR admission workflow tools from Curogram fix that gap.
We will show how SMS intake forms addiction treatment programs use can turn the admission into a clinical conversation, not a clipboard drill.
You will learn:
We will reference Curogram client data from clinical settings and the published Atlas Medical Center case study.
The goal is to give intake coordinators, admissions directors, and clinical leaders a clear picture of what better looks like.
Treatment should start with a face-to-face conversation. Not a stack of forms in a waiting room. Let's look at why the current intake workflow falls short, and what to do about it.
Opus EHR offers digital intake forms, which sounds like progress. The trouble is what happens after the patient hits "submit."
The data does not auto-populate into the patient record. Staff still have to retype every field by hand.
This section breaks down the daily cost of that gap. We will look at the workflow, the hidden errors, and what it does to the team.
Behavioral health intake is dense by design. CARF and Joint Commission standards call for full psychosocial assessments, consent forms, and substance use screening. For SUD treatment, 42 CFR Part 2 adds more consent steps on top.
A single admission packet often runs 19+ pages. That includes consent for treatment, consent for medications, medication lists, insurance cards, and emergency contacts. Each field has to be opened on one screen and typed into Opus on another.
Based on Curogram client data from clinical settings, manual re-entry takes 30 to 60 minutes per patient. Multiply that across 3 to 5 admissions a day. Half the morning is gone before any clinical work begins.
The lost hours are the obvious cost. The bigger risk is what slips through during the rush.
Medication reconciliation typos can affect psychiatric prescribing. A wrong insurance number can delay treatment authorization. In behavioral health, these are not small mistakes.
Intake coordinators were hired to coordinate care. Instead, many spend the day as data processors. That gap between job title and daily reality wears people out fast. Turnover follows.
The patient feels the friction too, even if they cannot name it. They walk into a program expecting support and structure. They find a lobby and another clipboard.
The first impression of treatment sets the tone. A digital admission paperwork behavioral health workflow that still feels paper-based sends the wrong signal. The patient sees a delay. The referring hospital sees a delay. The bed sits empty longer.
Here is what a typical Monday looks like for an intake coordinator without pre-arrival forms:
|
Time |
Task |
Clinical Work? |
|---|---|---|
|
9:00 AM |
Re-enter Patient 1 intake (55 min) |
No |
|
10:00 AM |
Re-enter Patient 2 intake |
No |
|
11:00 AM |
Field call from referring hospital |
No |
|
12:00 PM |
Re-enter IOP enrollment 1 |
No |
|
1:00 PM |
IOP group starts (paperwork still pending) |
Partial |
|
2:00 PM |
Re-enter Patient 3 intake |
No |
Zero clinical conversations. Zero patients greeted with a prepared file. The "digital" intake is digital in name only.
The good news: this is a workflow problem, not a clinical one. Pre-arrival intake forms SUD treatment programs use can solve it. The next section shows how.

The fix is simple in concept. Send the intake forms to the patient before they arrive. Let them fill everything out on their phone, at their own pace.
This section covers how Curogram delivers pre-arrival intake forms SUD treatment programs can rely on. We will also look at how it fits alongside Opus EHR without disrupting clinical workflows.
Curogram sends a text link to the patient's phone. They tap it, fill out the forms in a mobile browser, and submit. No app to install. No login to remember.
Text messages get opened. Most people read them within minutes. For SMS intake forms addiction treatment teams send, that open rate matters because admission is often a high-ambivalence moment.
Forms are fully custom. You can include ASAM screening elements, psychosocial assessments, medication lists, insurance card photo upload, and 42 CFR Part 2 consent. The format matches your accreditation needs, not a generic medical template.
Curogram does not try to replace Opus. The clinical record, e-prescribing, treatment planning, and billing all stay where they are.
Curogram handles the pre-visit form layer. Opus handles the clinical record. Secure patient intake Opus EHR integration means the form data is captured, organized, and ready for staff review before the patient walks in.
Most teams are live in days, not months. Staff training takes about 10 minutes. The change is quiet on the back end and dramatic on the front end.
Behavioral health and SUD programs carry extra privacy weight. Curogram is HIPAA-compliant and SOC 2 certified.
For SUD intake, the platform supports 42 CFR Part 2-compliant data handling from the first text message forward.
Here is how the workflow compares before and after:
|
Step |
Before Curogram |
With Curogram |
|---|---|---|
|
Form delivery |
PDF emailed or printed |
SMS link to phone |
|
Patient completes |
In lobby on clipboard |
At home, prior day |
|
Staff re-entry |
30 to 60 minutes |
Zero |
|
First interaction |
Paperwork |
Clinical conversation |
|
Bed confirmation to referrer |
Hours |
Minutes |
Many teams ask if Opus EHR intake form auto-population is possible natively. The honest answer based on user reports: not reliably for full admission packets.
Curogram fills that gap by capturing the data in a structured, organized format ready for staff to act on, removing the manual re-entry step that consumes intake coordinator time.
The point is not to replace Opus. The point is to make Opus easier to use at the moment when it matters most. Admission is the first clinical touchpoint. It deserves better than a clipboard.
When the forms come in before the patient does, the whole admission feels different. Staff is ready. The bed is confirmed. The first conversation is clinical, not clerical.
This section walks through what the "ready admission" looks like in real practice. We will cover the numbers, the team shift, and the patient experience.
Pre-visit form completion ties directly to appointment attendance. Patients who finish paperwork before arriving are more invested in showing up.
Based on our internal data, Atlas Medical Center reduced no-show rates from 14.20% to 4.91% in three months using Curogram tools. That is 3X better than the industry average.
For behavioral health, where ambivalence drives cancellations, removing the paperwork barrier removes one reason to back out.
Eliminating 30 to 60 minutes of re-entry per admission frees real hours. Intake coordinators can process 2 or 3 more patients per day without adding headcount. Across a month, that adds up to dozens of admissions.
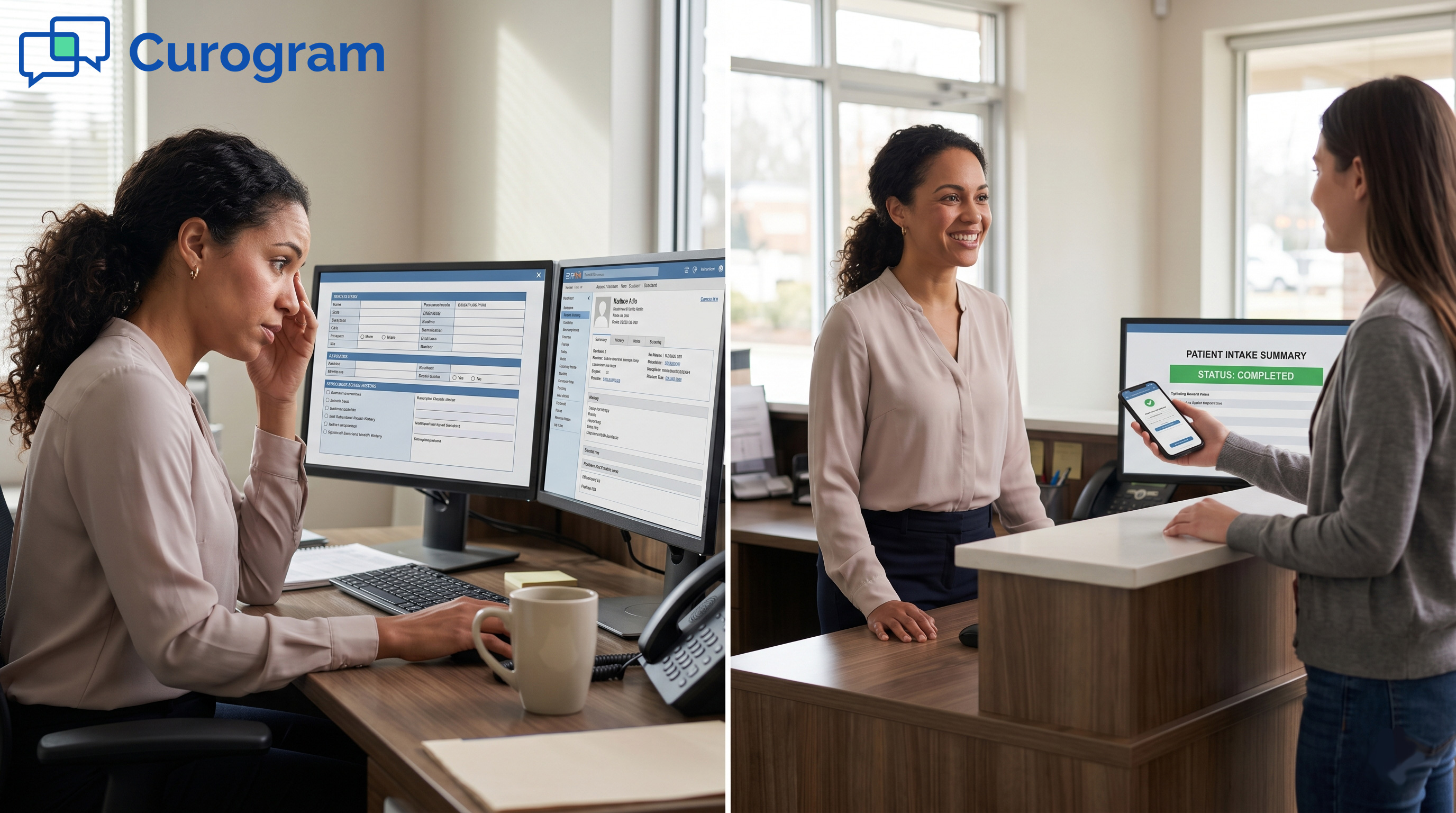
Picture the same coordinator from the first section. Same three residential admissions. Same two IOP starts. Different morning.
Each patient received an SMS link the day before. They filled out forms from home, at their own pace. When they arrive, the file is already populated.
The clinical work is still rigorous. Consent is still signed. Histories are still reviewed. The difference is when the data gets collected and who spends time on it. The patient does the data entry. The staff does the clinical work.
This is the bigger shift. Intake coordinators move from typing to talking. Admissions directors confirm beds in minutes, not hours. Referral sources get fast answers.
A patient walking into a program where staff already knows their story feels seen. The first impression is competence and care. That matters in behavioral health, where trust is the foundation of treatment.
People hired to support patients get to support patients. That is the job they signed up for. Job satisfaction goes up. Burnout slows down.
Here is the shift in plain terms:
|
Outcome |
Copy-Paste Admission |
Ready Admission |
|---|---|---|
|
Staff time per admit |
1 to 2 hours data entry |
15 min review |
|
First patient interaction |
Clipboard |
Clinical conversation |
|
Bed confirmation speed |
Hours |
Minutes |
|
Data entry errors |
Frequent |
Rare |
|
Daily admit capacity |
3 to 5 |
6 to 8 |
Not every patient owns a smartphone. Curogram forms open in any mobile browser, so basic phones work, too.
For patients with no phone access, staff can complete the same form on-site, keeping the data structure consistent.
The ready admission is not a vision. It is a workflow shift that programs are running today. The tools exist. The compliance is built in. The only thing left is to use them.

Behavioral health admission is the first real touchpoint of treatment. It sets the tone for everything that follows.
It deserves more than 19 pages of re-typed paperwork.
This blog has walked through the gap, the fix, and the shift. Let's pull it together in one view.
Opus EHR is a strong clinical platform. Its digital intake forms collect data, but that data does not auto-populate into the patient record. Staff fills the gap by hand.
That gap costs hours per admission. It also costs accuracy, staff morale, and patient trust. Errors in medication reconciliation or insurance details create downstream problems that ripple through the whole treatment episode.
Curogram delivers digital behavioral health intake forms Opus EHR admission workflow teams need. The forms arrive by SMS link along with reminders before the patient does. The patient fills them out on their phone.
The platform is HIPAA-compliant and supports 42 CFR Part 2 data handling. Forms are custom-built for behavioral health and SUD intake. Implementation takes days, and staff training is short.
Intake coordinators stop being data processors. They start being patient advocates. Admissions directors confirm beds in minutes. Referral sources get fast answers.
Patients arrive feeling prepared, not overwhelmed. The first interaction is a clinical conversation. That is what "the ready admission" looks like in practice.
Based on Curogram client data from clinical settings, the gains are real:
Admission should start with care, not clerical work. The first conversation should be about the patient, not their paperwork. That is the shift worth making.
Your intake team did not sign up to copy and paste 19 pages of patient data. Your patients did not walk through your door to fill out another clipboard. The tools to fix that exist today.
The clipboard era is ending. The ready admission is already here.
Opus EHR is for your clinical documentation. Curogram is for your patient's first impression. The two work together, and the workflow shift is real.
If you run a behavioral health or SUD treatment program on Opus EHR, the path forward is short. See how pre-arrival intake works for your team in a 15-minute demo.
Book a Demo to see Curogram in action with Opus EHR. Bring your toughest admission scenario and we will show you how it would run differently.
💡 Opus EHR handles clinical notes well, but its intake forms have a gap. Patient data does not auto-populate into the chart. Staff must copy and...

💡 The patient intake experience for Opus EHR behavioral health programs through mobile forms with no portal requirement changes on the first day of...

💡 Imaging centers using StreamlineMD process dozens of patients each day. Paper intake forms slow things down. Curogram's digital intake forms for...