
 Jo Galvez
Jo Galvez
Digital Intake Forms for Opus EHR: End 19-Page Copy-Paste Admission
💡 Digital behavioral health intake forms Opus EHR admission workflow tools fix a known gap. Opus EHR offers digital intake forms, but the data does...
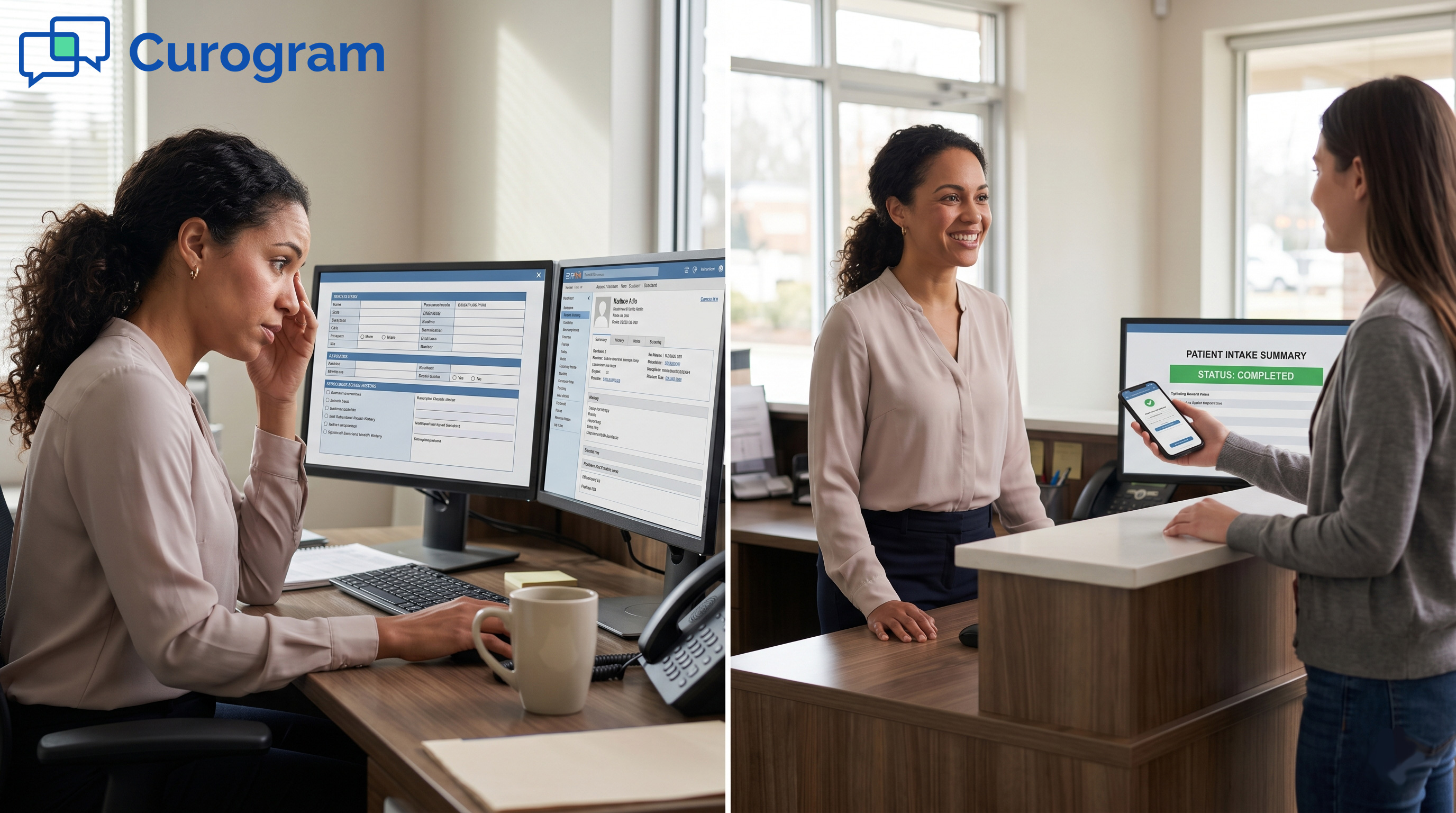
It’s Monday, and three new patients are due for residential intake. The first one has already filled out 19 pages of forms online over the weekend.
And yet, the intake coordinator is still typing.
She opens the digital form on one screen. The Opus chart sits on the other. Then she begins the slow march.
Name. Date of birth. Address. Insurance ID. Medication list. Substance use history. Trauma screen. Emergency contacts.
Field by field. Line by line.
By the time she finishes, 53 minutes have passed. The second patient is in the lobby. The third has not been called back yet. A referral source has already left two voicemails.
This is the quiet bottleneck inside many SUD treatment programs that run on Opus EHR. The forms are digital. The data is digital. But the bridge between them is still a human typing the same data twice.
That is the problem this blog tackles. We will look at why the re-entry step exists, what it costs your team each day, and how SMS-delivered forms close the gap. We will also share what changes for intake staff once the typing stops.
The promise is simple: the admission begins with a clinical conversation, not a clipboard.
Opus EHR is a strong clinical platform. It tracks treatment plans, progress notes, and billing well. But the intake side has a known gap that frustrates many teams.
The forms exist. Patients can fill them in. The issue lies in what happens next.
When a patient fills out an Opus intake form online, the answers do not auto-populate into the patient record.
The form output is more like a static document. Staff still need to read it, then type each answer into the chart by hand.
For a routine primary care visit, this might cost 10 minutes. For a behavioral health admission, it is a different story.
SUD treatment intake is dense. A single admission can include consent forms, a psychosocial assessment, trauma screens, substance use history, medication reconciliation, and insurance verification.
That stack often runs 19 pages or more. Every page has fields. Every field has to land in the correct spot inside Opus. One typo on an insurance ID, and a claim gets rejected weeks later.
Intake coordinators did not pick this career to type. They picked it to help people in a hard moment. Yet half the day gets pulled into copy-and-paste work that a phone in the patient's pocket could already handle.
Based on our internal data, healthcare practices often manage 80 or more calls a day on top of paperwork. Add a 19-page intake packet per admission, and the math stops working.
Picture three admissions on a busy Monday. Each one takes 30 to 60 minutes of pure re-entry. That is 2 to 5 hours of staff time gone before lunch. None of it is clinical work.
While the coordinator types, the lobby fills up. Phones ring. Referral partners wait for bed confirmations. The pace slows the whole program.
This is where reducing intake data entry in SUD treatment becomes more than a slogan. It is a daily survival need for any program that wants to grow its census without burning out its front office.
Errors slip in when humans transcribe under pressure. A wrong digit on a policy number can delay billing for weeks. A misspelled medication can spark a safety risk in the first clinical review.
These are not edge cases. They are normal outputs of a workflow that asks people to be perfect typists at 9 a.m. on a Monday.
The patient sees a lobby. They see a clipboard pushed across the desk, even though they filled out the same forms last night. They start to doubt the program before treatment begins.
First impressions matter most when a patient is on the fence about staying. The intake desk is where ambivalence either softens or hardens.

The fix is not to replace Opus. The clinical record stays where it is. The fix is to add a layer that handles the pre-arrival forms in a smarter way.
That layer is Curogram. It sits next to Opus and removes the re-entry step from the admission. Here is how that looks day to day.
A new patient is scheduled for admission on Monday. On Friday, the staff sends a secure SMS link and a reminder. The patient taps it on their phone, fills in the forms at home, and saves their progress between sittings if needed.
By Monday morning, the chart is ready for review. The 53-minute marathon becomes a 5-minute scan. That shift is the heart of the intake form automation behavioral health Opus teams have been asking for.
They get a short text. They tap a link. The forms open in their mobile browser, sized for a small screen. They can pause, look up a med name, then return.
No printer. No clipboard. No waiting room paperwork while feeling shaky on day one.
Coordinators get a notice when forms are done. They open Opus, pull the structured data, and review for accuracy. They flag any insurance gaps before the patient arrives, not during the visit.
Generic patient forms do not fit SUD work. The forms need to cover trauma history, substance use timelines, prior treatment episodes, and consent for medication. Curogram supports all of it through fully custom templates.
Long forms are normal in behavioral health. The platform handles them through mobile-first design and progress saving.
A patient can fill out 19 pages across a Friday night and a Saturday morning, then submit.
This matters for digital admission forms addiction treatment Opus EHR programs run, because partial completion is often the rule, not the exception.
The forms are HIPAA compliant. For SUD work, the platform supports the stricter 42 CFR Part 2 handling that protects substance use records. Sensitive history stays on a secure channel from the first touchpoint.
The shift is easier to see in a side-by-side. Here is what changes once SMS forms are in place.
|
Workflow Step |
Before SMS Forms |
After SMS Forms |
|
Form delivery |
Paper packet at the desk |
Secure SMS link sent days early |
|
Patient setting |
Lobby, under pressure |
Home, at their own pace |
|
Staff re-entry |
30 to 60 min per admission |
5 min review per admission |
|
Errors |
Typos, missed fields |
Patient-typed, fewer transcription errors |
|
Admission length |
2 plus hours |
About 45 min |
The pattern is clear. Move the typing off the staff and onto the source: the patient and their own phone.
The point of this shift is not just speed. It is what your team can do with the hours you give back. Below is what we see most often once the re-entry step is gone.
When the form work moves off the desk, the role of the intake coordinator changes. They stop being the bottleneck. They start being the first face of the program.
This is the core of the intake coordinator workload reduction that behavioral health leaders want, without cutting staff or skipping steps.
With data pre-loaded, the coordinator can spend the first 15 minutes greeting the patient instead of typing. They can flag risk items for the clinical team before the assessment starts.
That early read can shape the rest of the day. A patient who feels seen at 9 a.m. is easier to engage at 10.
Staff can return calls from referral sources within the hour. They can chase down prior authorizations the same day. They can confirm beds while the lead is still warm.
This is how streamline admission workflow Opus EHR behavioral health programs turns into real bed growth, not just a faster intake form.
Referral sources do not pick favorites by accident. They pick the program that calls back first and confirms a bed by the end of the day.
When admission processing time Opus EHR programs drops from two hours to forty-five minutes, the whole referral funnel speeds up. Beds turn over faster. Confirmations land sooner. The phone rings more.
Say a program does four admissions a day. Each one saved 45 minutes. That is three full hours of staff time, every day, that can move to outreach and follow-up.
Now run that across a month. The same team can take on more admissions without adding a single new hire.
Pre-visit form completion correlates with stronger commitment. Atlas Medical Center cut no-show rates from 14.20% to 4.91%, a result 3X better than the industry average, based on our internal data. Patients who finish paperwork before arrival are simply more likely to walk through the door.
Monday again. Three admissions on the board. All three filled out forms on Saturday. The coordinator gets in at 8 a.m. and reviews all three charts in 15 minutes.
She flags one insurance issue and makes one call. By 9 a.m., the first patient walks in and is greeted, not parked. By noon, all three admissions are clinically engaged.
By 1 p.m., she is on the phone with two new referral leads. The morning that used to be a five-hour data entry session is now a morning of patient care and growth.
That is what Opus EHR intake coordinator efficiency looks like when SMS forms remove the typing from the admission.

Opus EHR was built for clinical work. It tracks the course of treatment well. The intake side, though, still leans on people to do work that machines can handle.
That gap is small on paper. In daily life, it eats hours and burns out staff.
The fix is not a new EHR. It is a layer that closes the gap between the form and the chart.
Opus EHR holds the clinical record. Curogram holds the pre-arrival forms. Together, they remove the copy-paste step that slows every admission.
Your coordinators stop being typists. They start being the first clinical contact a patient meets.
Behavioral health programs face rising demand and tight staffing. There is no slack left in most front offices. Every hour saved on data entry is an hour that can move to patient care or census growth.
Programs that fix the intake bottleneck early will pull ahead. Programs that do not will keep paying the cost in burnout, errors, and lost referrals.
A demo is not a sales pitch. It is a 15-minute look at the workflow inside your own program.
You will see how a 19-page intake packet gets sent through SMS, how the patient fills it out on a phone, and how the data shows up before the visit. You will also see what the 5-minute review looks like in practice.
The admission is the first clinical moment of treatment. It sets the tone for everything after.
If your team spends that moment typing, the patient learns the wrong lesson on day one. If your team spends it greeting, listening, and preparing, the patient learns the right one.
Your intake coordinators deserve to spend their days welcoming patients, not re-entering data that already exists.
Book a Demo with Curogram and see how SMS-delivered intake forms work alongside Opus EHR.

💡 Digital behavioral health intake forms Opus EHR admission workflow tools fix a known gap. Opus EHR offers digital intake forms, but the data does...

💡 The patient intake experience for Opus EHR behavioral health programs through mobile forms with no portal requirement changes on the first day of...

💡 Imaging centers that streamline imaging center intake workflows can cut check-in time from 15 minutes to under 3 minutes per patient. Curogram’s...