
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
How to Switch from Weave to Curogram: Complete Migration Guide
💡 A switch from Weave to Curogram migration moves your practice off VoIP-centric infrastructure and onto a medical-first clinical automation...
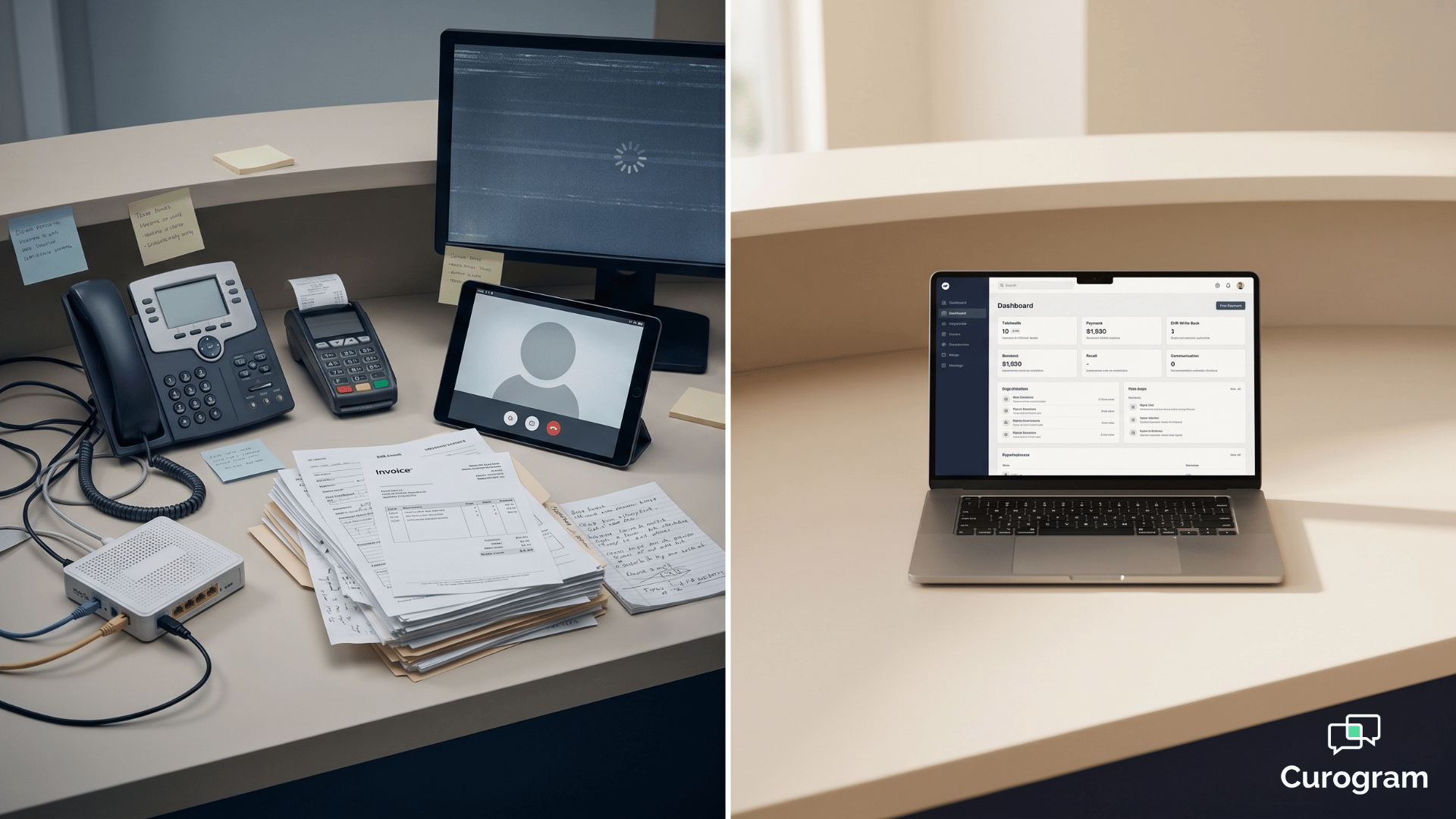
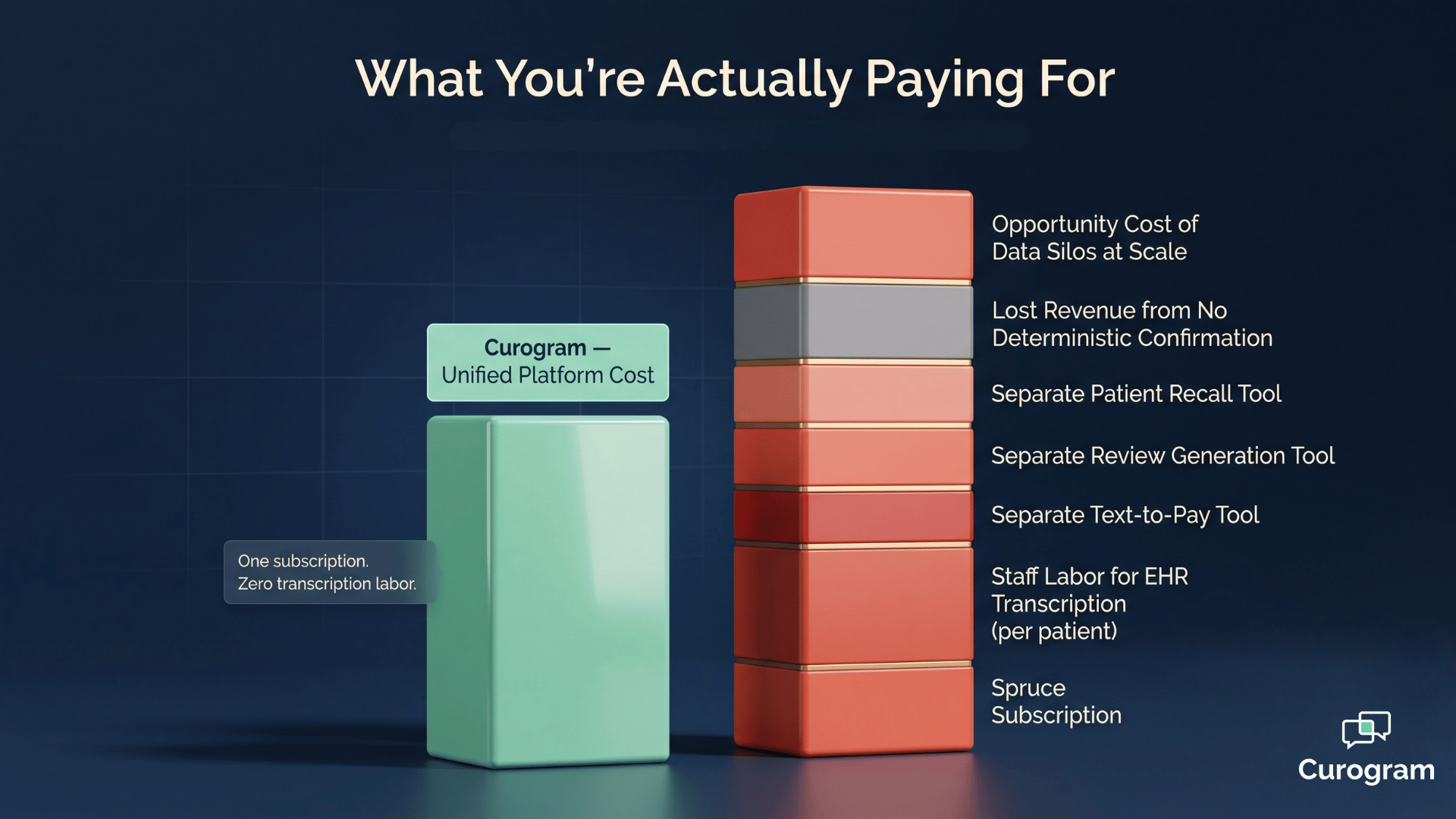
Imagine paying for a patient engagement platform every month—and still asking your front desk to retype every call into the EHR. The phone rings. A name pops up on screen. Staff smile, talk, schedule, hang up. Then the real work starts.
That second job, the one nobody priced into the contract, is where the budget quietly bleeds. It happens after every call. After every text. After every form.
This is the part of the patient engagement platform ROI phone system vs clinical automation debate that sales decks skip. The sticker price looks reasonable. The total cost of running it inside a medical practice does not.
For practices weighing weave vs curogram pricing value medical decisions, the math is rarely about software fees. It is about VoIP desk phones on every workstation.
ISP upgrades to keep calls clear. Hardware payment terminals. And the staff hours spent doing what the platform was supposed to do for them.
Then there is the revenue you never see. The no-show that wasn't confirmed. The recall patient who never got a follow-up. The review that never got asked for.
Each one is small. Together, they decide whether your platform pays for itself or quietly drains your margin.
This guide breaks down the curogram weave cost comparison roi question the way a CFO would. We will look at hardware. Hidden labor. Reliability. Revenue recovery. And we will use real numbers from real practices to show you what the gap actually looks like in dollars.
By the end, you will know whether your communication hub is working for you—or whether it is the most expensive line item you forgot to count.
The most expensive patient engagement platform is not the one with the highest monthly fee. It is the one that creates the most manual work, needs the most hardware, and delivers the least automation per dollar.
Phone-centric platforms carry a unique burden in medical environments. They were built for dental offices and small businesses where the front desk lives on the phone.
That model does not match how a modern medical practice actually runs.
Think about your last hour at the clinic. Patients texted to reschedule. Forms came in through a portal. A telehealth visit ran in the background. Maybe two or three actual phone calls happened.
The phone is one channel out of many—not the center of the universe.
When the platform assumes otherwise, costs compound in four places:
Each of those gaps shows up later in this guide with real numbers behind it. Together, they shape the real economics of choosing between a communication hub and a clinical workflow engine.
Weave's design imposes a category of cost that does not appear on the invoice. Call it the VoIP infrastructure tax. It is the cumulative price of running a phone-system platform in a 2026 medical environment where cloud-native automation is the standard.
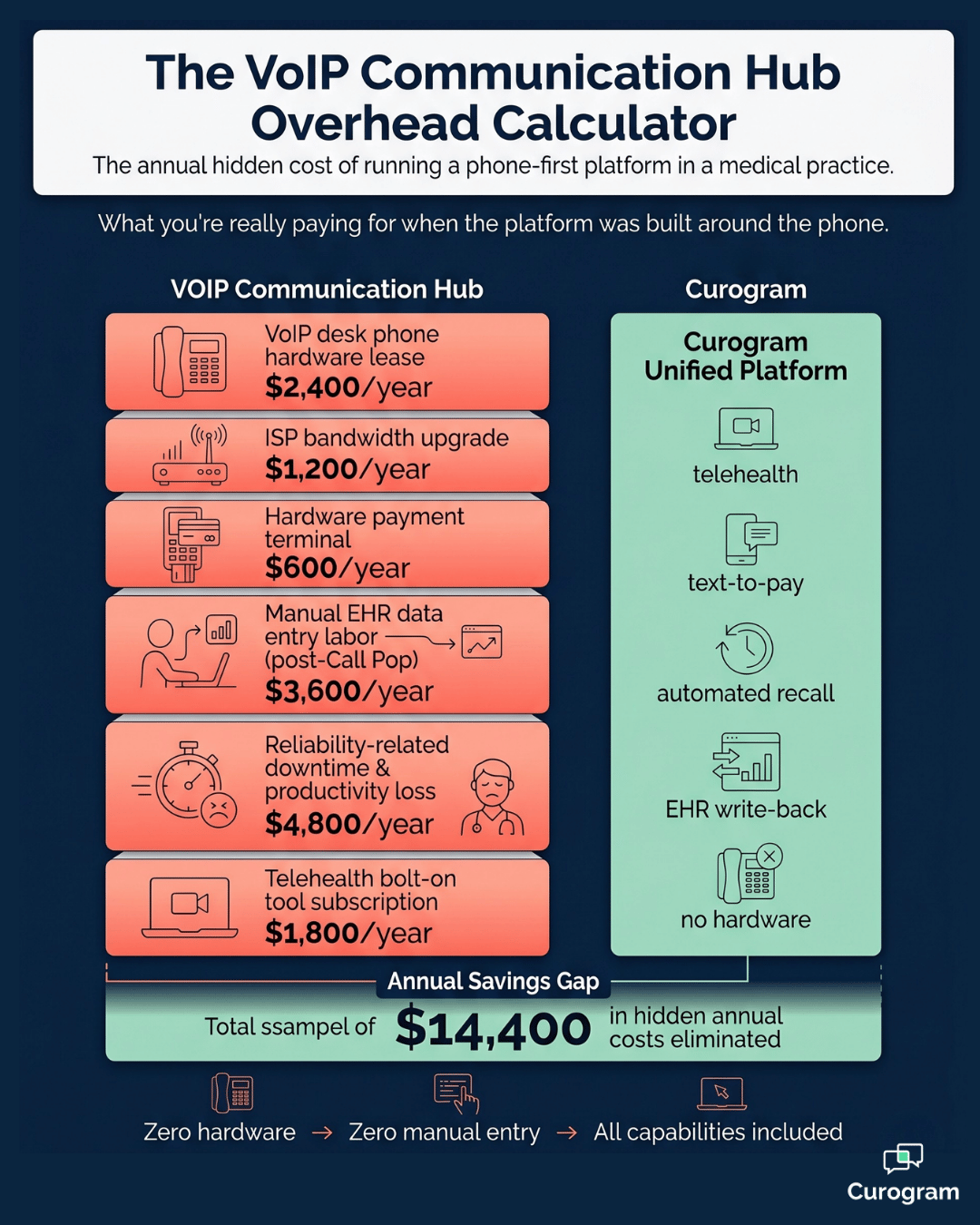
The most visible piece is hardware. Weave typically requires proprietary desk phones, hardware payment terminals, and ISP bandwidth strong enough to support reliable VoIP across every workstation. These are capital expenses up front and recurring expenses forever after.
For context, a mid-sized practice with 8 workstations may spend 3,000 to 6,000 dollars on desk phone hardware alone.
Add a payment terminal and an ISP upgrade, and the first-year VoIP hardware cost medical practice burden can climb past 8,000 dollars before a single text is sent. Cloud-native platforms eliminate that line entirely.
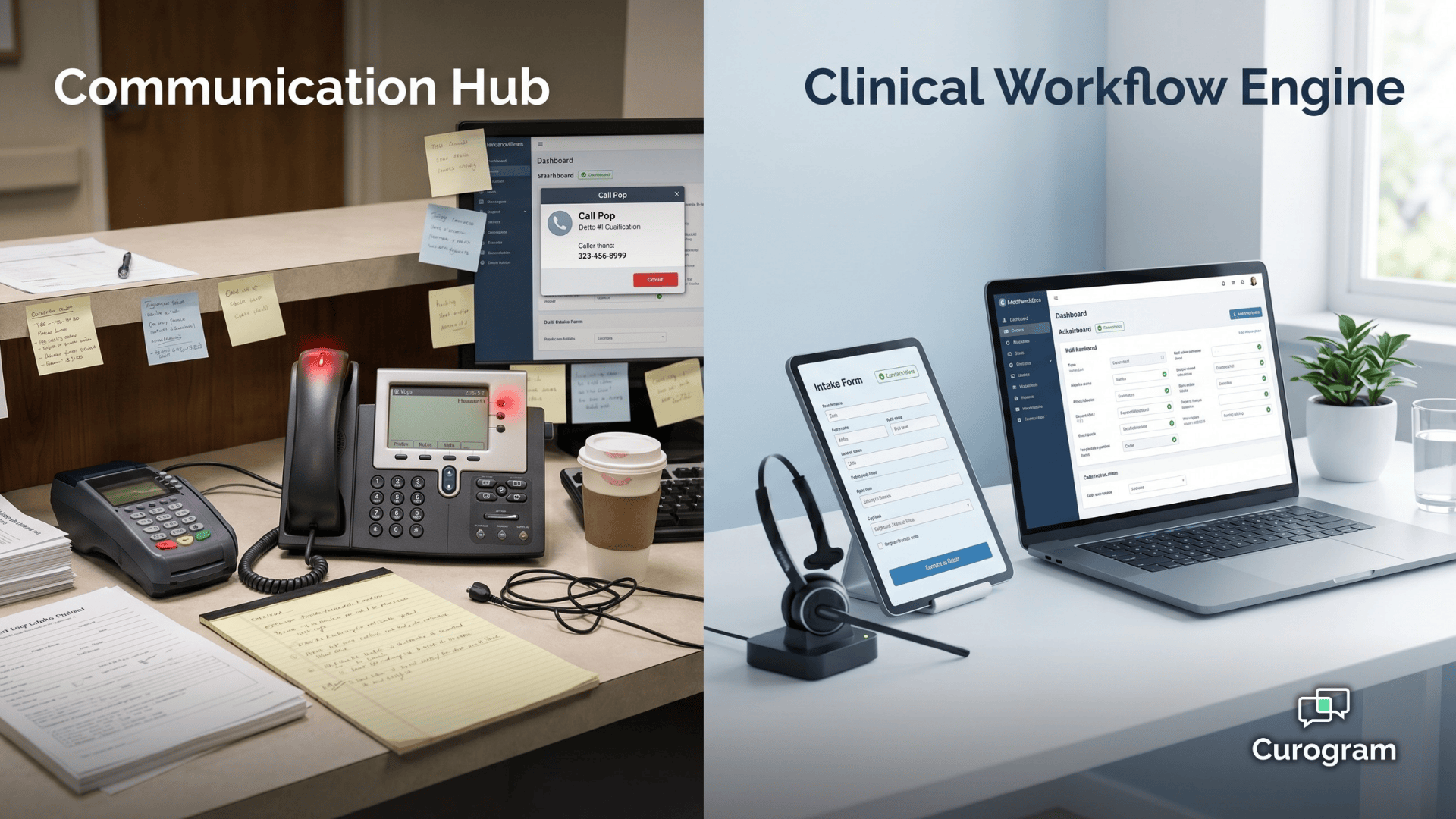
The less visible cost is bigger. Weave's Call Pop shows you who's calling. After the call, your staff still has to open the EHR and type in what just happened.
Now scale that. A practice handling 40 patient interactions a day that generate clinical data is looking at roughly 1 to 2 hours of daily manual entry. That is 5 to 10 hours a week per front desk staff member. Across a year, it adds up.
Here is what that looks like in dollars at a 22 dollar-per-hour loaded labor rate:
| Daily entry hours | Weekly hours | Annual hours | Annual labor cost |
|---|---|---|---|
| 1 hour | 5 hours | 260 hours | 5,720 dollars |
| 1.5 hours | 7.5 hours | 390 hours | 8,580 dollars |
| 2 hours | 10 hours | 520 hours | 11,440 dollars |
This means:
Even on the conservative end, a practice loses nearly 6,000 dollars a year to data entry that deep clinical integration would automate—well above typical medical practice cost efficiency benchmarks.
For your team, those hours could go to patient care, follow-ups, or collections.
There is a third layer most weave total cost VoIP phone system healthcare reviews miss. Verified user reviews flag dropped calls, frozen phones, and system glitches. Each one steals a few minutes here, a few minutes there. It adds up to hours per week of lost productivity.
Then there is telehealth. Weave does not include native virtual care, so practices either bolt on a separate tool or skip telehealth entirely. Either way, you pay—in another subscription or in lost visit revenue.
Curogram clears all of this in one sweep. There is no hardware to buy, no Call Pop entry to clean up, and no second tool for telehealth. The platform runs cloud-native on whatever device your team already uses, with bi-directional API write-back that keeps the EHR current without staff effort.
Costs are only half the story. The other half is what your platform earns back. This is where the no-show revenue recovery communication hub vs automation gap shows up clearest.
Most practices lose 20,000 to 30,000 dollars a month to no-shows. Curogram users see deterministic confirmation rates above 75%.
The reason that number holds up is automatic EHR write-back—the confirmation does not just sit in a dashboard, it updates the chart.
The numbers tell the story. Atlas Medical brought its no-show rate from 14.20% down to 4.91% in three months. That is a 65% drop.
For a practice billing 200 dollars per visit and seeing 800 visits a month, recovering 9% of those visits is roughly 14,400 dollars a month, or 172,800 dollars a year.
Covina Arthritic Clinic sends more than 1,100 automated confirmations every month, and staff cost stays flat as patient volume grows. The platform scales. The headcount does not.
Beyond no-shows, Curogram opens revenue streams a VoIP communication hub was not designed to support:
For your team, that means revenue that compounds. Reactivated patients, faster collections, and a steady stream of reviews that bring in new bookings—all without adding staff.
That compounding effect is exactly what shows up next when you look at total cost of ownership side by side.

Pricing pages tell you what the software costs. They do not tell you what the platform costs to operate. This breakdown covers both.
| Cost Dimension | Curogram | Weave |
|---|---|---|
| Hardware Requirements | None; entirely software-based and device-agnostic | VoIP desk phones, hardware payment terminals, ISP upgrade |
| Manual EHR Data Entry | None; bi-directional API with discrete field write-back | Required after every interaction; Call Pop displays but does not write data |
| System Reliability Cost | Cloud-native; enterprise-grade uptime; ISP-independent | VoIP-dependent; dropped calls and glitches create productivity loss |
| No-Show Revenue Recovery | 53% lower rate; 75%+ confirmation; auto EHR write-back | Reminders sent; limited clinical write-back in medical EHRs |
| Payment Collection | Native text-to-pay; no hardware required | Integrated payments; hardware terminal dependent |
| Telehealth | Native virtual waiting room; no additional cost | Not a native capability; separate tool required |
In practice, this means the comparison is not subscription vs. subscription. It is one all-inclusive medical platform vs. a stack of subscriptions, devices, and labor hours.
The wider your patient volume, the wider that gap gets.

A 4-provider practice and a 12-provider practice may pay similar Weave subscription tiers, but the larger one absorbs far more of every hidden line item—more workstations needing phones, more daily interactions needing manual entry, more dropped-call minutes spread across more staff.
That scaling pattern is exactly why architecture, not subscription price, decides the long-run economics.
For medical practices doing a real economic review, the total cost of a VoIP communication hub adds up fast.
Every desk phone. Every ISP upgrade. Every manual EHR entry hour. Every minute of productivity lost to a glitchy system. Every dollar of revenue the architecture cannot capture.
These costs do not stay flat. They compound, mirroring trends in rising healthcare operational costs and system inefficiencies.
They grow with patient volume, which means phone-centric platforms get more expensive to run, not less, as your practice scales.
Curogram delivers the inverse economics by design. The shift shows up across four dimensions at once:
The upgrade from a communication hub to a clinical workflow engine is not a tech preference.
For most growing medical practices, it is a financial decision that pays back in months, not years—and it sets up the operating model the next section turns into a concrete next step.
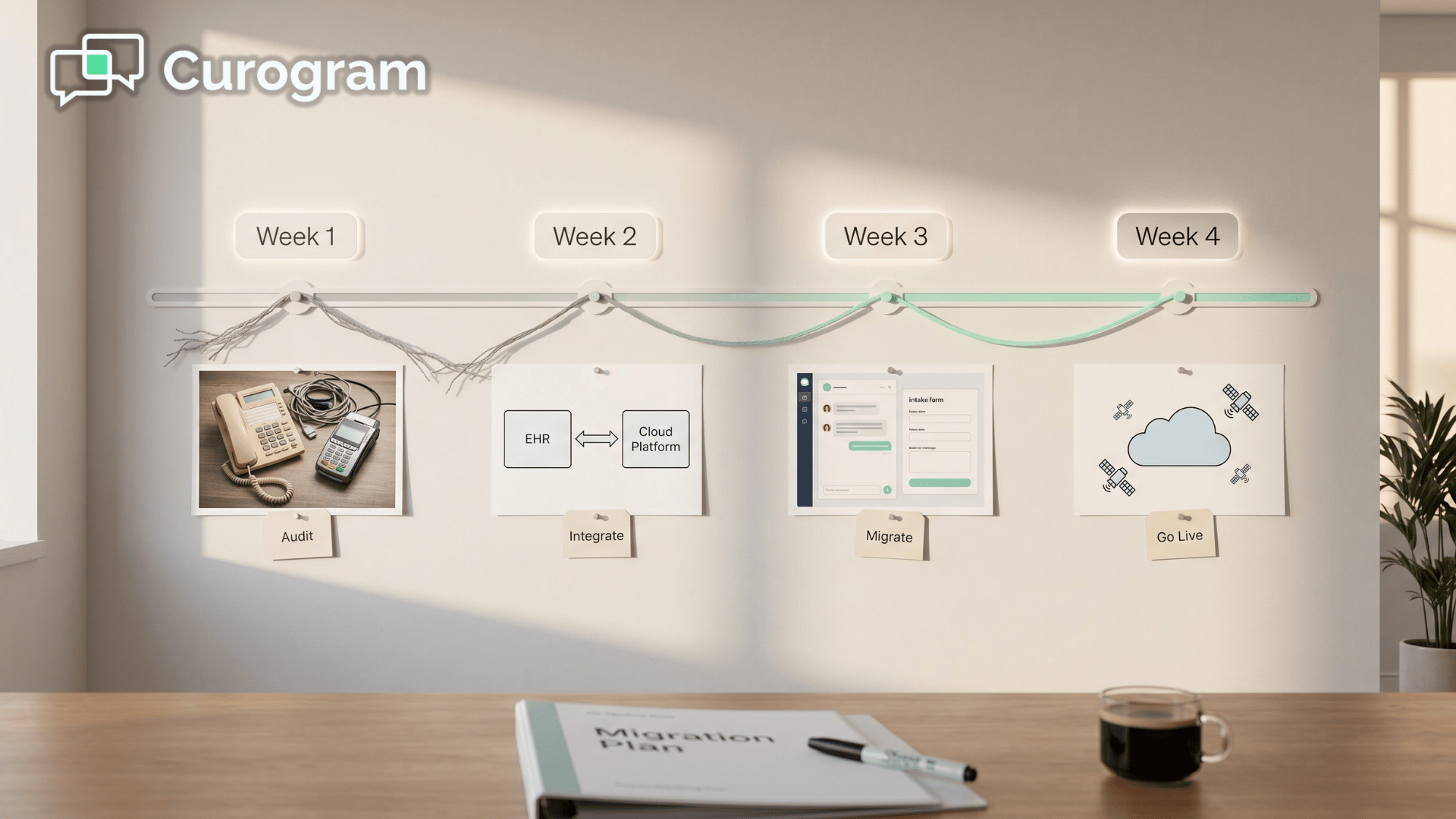
The hardest part of any platform decision is seeing the real cost before you sign. Sticker price is easy. Hidden labor, hardware leases, and missed revenue are not.
A 30-minute Curogram demo gives you that visibility. We will walk through your patient volume, your current no-show rate, and the manual hours your team spends on EHR cleanup after each interaction.
Then we will model what those numbers look like running on a medical-first platform.
Most practices we talk to are surprised twice.
First, by how much they were quietly spending on VoIP infrastructure and manual entry.
Second, by how much revenue they were leaving on the table from no-shows, unbilled recalls, and paper-based collections.
You will leave the demo with a plain-English breakdown of your estimated annual VoIP infrastructure tax, your projected no-show recovery based on current rates and visit value, and a side-by-side ROI view comparing current setup with Curogram.
No pressure. No long-form RFP. Just numbers built around your practice.
If a 53% no-show reduction, 75%+ confirmation rates, and zero hardware sounds like it would change your spreadsheet, this is the easiest next step you can take. Bring your patient volume, your average visit value, and any frustrations with your current tool. We will handle the rest.
The practices doing this review now are the ones positioning themselves to grow without growing overhead.
Whether Curogram is the right fit or not, you will leave with a clearer picture of what your platform is actually costing you—and what a medical-first alternative could return.
Schedule a demo today and see the full curogram weave cost comparison roi breakdown for your practice in under 30 minutes.
💡 A switch from Weave to Curogram migration moves your practice off VoIP-centric infrastructure and onto a medical-first clinical automation...
💡 Curogram and Weave take different paths to patient engagement. Curogram is built around clinical workflow automation, meaning confirmations,...
💡 A curogram spruce cost comparison roi analysis shows that subscription pricing is the smallest expense. The biggest cost is the labor needed to...