
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
How to Switch from Weave to Curogram: Complete Migration Guide
💡 A switch from Weave to Curogram migration moves your practice off VoIP-centric infrastructure and onto a medical-first clinical automation...

Think about the last time a patient confirmed their appointment through your automated reminder. Did that confirmation automatically update in your EHR — or did someone on your front desk have to log it manually?
If you're still manually bridging the gap between what your communication platform displays and what your EHR actually contains, you're experiencing an integration problem.
Not a workflow problem. Not a staffing problem. An integration problem.
It sounds like a subtle distinction. It isn't.
Medical practices evaluating communication platforms tend to compare features:
Reminders, two-way texting, telehealth, digital intake forms. But the capability that determines how much time your staff saves — or doesn't — isn't on the feature checklist. It lives in how deeply the platform connects with your EHR.
There are two fundamentally different integration models in this market.
One treats your EHR as a data source to display information on a screen. The other treats it as a living clinical record to be read, updated, and maintained in real time — without anyone touching a keyboard.
That difference has a direct, measurable impact on your staff hours, your no-show rate, and your revenue.
When you look closely at curogram weave ehr integration architecture, the technical differences go far deeper than any product brochure reveals.
Weave is a VoIP phone system at its core. It connects to practice management systems through middleware — a layer that reads surface-level data like patient names, appointment times, and phone numbers to display them when someone calls.
That's a genuinely useful feature called Call Pop. But it is not clinical integration.
Curogram is built on an entirely different model. It connects to your EHR through a continuous, cloud-native REST API that reads and writes clinical data at the field level — in real time, without staff having to manually intervene.
When a patient submits intake information, it maps to the right EHR field. When they confirm an appointment, your schedule updates automatically.
This article breaks down exactly how these two models differ — technically, operationally, and financially.
Because the architecture underneath the interface matters more than most practices realize before they've already signed a contract.
Healthcare EHR integration isn't binary. It exists on a spectrum — from surface-level data reads that power a caller ID screen, to deep bi-directional APIs that write structured clinical data directly into discrete EHR fields.
Where a platform sits on that spectrum determines the scope of automation it can actually deliver.
Think about what your staff handles in a single morning.
Each interaction type generates data that needs to land accurately in your EHR:
In each case, the question isn't whether your platform collects that data. It's whether it moves that data all the way into the right EHR field automatically — or whether your staff still has to finish the job.
That gap — between what a platform displays and what the EHR contains — is where manual work lives. And for practices processing hundreds of patient interactions per month, even a few minutes of manual entry per interaction adds up fast.
Consider a practice handling 500 patient touchpoints per month, each requiring just 3 minutes of manual EHR bridging.
That's 25 hours per month spent not on patients, but on transcription.
The depth of integration is the variable that changes this equation. Platforms built on true bi-directional clinical APIs eliminate that manual step entirely. Platforms built on middleware scraping — by design — do not.
Understanding which category your current or prospective platform belongs to is the first step toward an informed evaluation of curogram weave ehr integration architecture.
Curogram's EHR connection runs on a modern REST API with continuous, real-time data exchange in both directions.
The platform reads from your EHR — pulling patient demographics, schedules, and clinical data — and writes back to the EHR with confirmation status, intake responses parsed into discrete fields, and demographic updates.
None of that requires a staff member to manually process the information.
This is a clinical-first integration model built to handle the data complexity of medical specialties.
Unlike basic PMS environments, medical EHRs require handling structured data across multiple dimensions:
These aren't simple data points, and Curogram's API is designed to handle that depth without flattening it into unstructured text that someone else has to sort out later.
The result is a closed-loop data cycle: patient input goes in enabled by secure patient messaging, the EHR record gets updated, and staff confirmation workflows get bypassed entirely.
Weave's integration architecture reflects its origins as a VoIP telephony platform.
The core technology is middleware that scrapes data from your Practice Management System to populate its Call Pop feature — displaying caller information on screen during incoming calls so your team knows who's calling and what their appointment status is before they say hello.
For dental and veterinary PMS environments, where the data set is relatively simple (name, appointment time, phone number), this approach works well. The clinical complexity just isn't that high.
But in medical EHR environments — where intake involves medication histories, multi-condition flags, insurance verifications, and specialty-specific clinical fields — middleware scraping cannot achieve the depth or the write-back capability that clinical automation requires.
This is the core tension behind the bi-directional API vs VoIP middleware scraping debate.
Weave excels at data display, as reflected in user reviews. Curogram excels at data movement.
For medical practices, the distinction defines what your staff has to do after the platform does its part.

Most integration conversations focus on what a platform can read from the EHR. The more operationally important question is what it can write back. And on that dimension, the gap between these two platforms is significant.
Curogram's bi-directional API writes discrete data into specific EHR clinical fields. Intake responses map to allergy fields, medication lists, and clinical history. Appointment confirmations update scheduling status. Demographic changes sync in real time.
The platform completes the clinical data cycle — from patient input to EHR record — without any staff stepping in between.
Weave's middleware model does not provide equivalent discrete write-back for medical EHRs. Call Pop is a display feature — it shows data during a call, but it does not process or return that data to the EHR after the interaction ends.
When a patient provides clinical information through Weave, the manual work still lands on your team.
Staff typically have to:
This is the practical consequence of weave call pop PMS sync limitations medical EHR practices experience once they move past the demo stage.
It's not a product flaw — it's a design consequence.
Weave was built for VoIP telephony, not clinical data management. For a dental practice running a straightforward schedule, that's fine. For a medical group handling 1,000+ appointment interactions per month across multiple specialties, it means your front desk is doing the work the platform should be doing.
The real-world impact of discrete write-back is measurable.
Atlas Medical reduced its no-show rate from 14.20% to 4.91% within three months of implementing Curogram — a result that depended entirely on confirmation responses automatically updating the EHR in real time.
Covina Arthritis Clinic now processes more than 1,100 automated monthly confirmations, each of which writes directly to the scheduling system without staff involvement.
To put that in concrete terms: if your practice sees 300 appointments per week and your no-show rate drops by even 5%, that's 15 recovered appointments per week.
At an average visit value of $150, that's $2,250 per week — or roughly $117,000 in annual recovered revenue.
That outcome isn't achievable with a read-only display layer. It requires the EHR to be updated in real time, automatically, every single time a patient responds.
Weave EHR write-back in a medical practice context simply cannot complete that cycle. Curogram can.

The table below compares both platforms across the dimensions that matter most for medical practices evaluating weave middleware integration enterprise EHR environments against a cloud-native clinical API.
| Dimension | Curogram | Weave |
|---|---|---|
| Architecture Model | Cloud-native REST API; clinical-first design | VoIP middleware; PMS data scraping |
| Data Direction | Bi-directional: continuous read and write | Primarily read-only; limited write-back in medical EHRs |
| Write-Back Depth | Discrete field-level (allergies, meds, history, appointment status) | Surface-level; Call Pop display only; manual EHR update required post-interaction |
| Target Ecosystem | Medical specialties and enterprise EHRs | Dental, veterinary, and optometry PMS environments |
| Infrastructure Dependency | Cloud-native; no local hardware required | VoIP/ISP-dependent; proprietary phone hardware required |
| Data Complexity Supported | Multi-specialty clinical fields, medications, history | Basic PMS data: name, appointment time, phone number |
| Sync Timing | Real-time, continuous | Periodic; dependent on middleware polling frequency |
| Staff Manual Entry Required | No — full automation to EHR field level | Yes — staff must update EHR after clinical interactions |
For medical practices, not every row in this table hits equally.
The dimensions that most directly affect daily operations are:

Those three dimensions define whether your staff spends their day on patients or on data cleanup.
Curogram answers all three differently — and more favorably for medical complexity — than Weave does.
Medical practices operate at a level of data complexity that surface-level PMS sync was never designed to handle.
Consider what a typical patient visit actually requires your systems to process:
A platform whose integration reads basic appointment data to display on a phone screen cannot automate these workflows. It can only make the phone call that precedes the manual data entry slightly more convenient.
This is the core challenge of evaluating a VoIP platform vs cloud-native clinical integration for a medical group. A VoIP platform built for small dental offices was designed to solve a different set of problems — and it solves them well.
But when you layer that model onto a medical enterprise with clinical data requirements, the middleware wasn't built for that environment, and the limitations surface quickly.
Curogram's cloud-native API is built for medical data complexity from the ground up.
When your integration reads and writes discrete clinical data at the field level, intake resolves without transcription. Confirmations are always reflected in the EHR.
Staff never needs to manually bridge the gap between what the platform shows them and what the EHR actually contains.
The operational impact compounds over time. A practice that automates 1,000 monthly confirmations and eliminates 3 minutes of manual EHR entry per confirmation saves roughly 50 hours per month.
At a burdened labor cost of $25 per hour, that's $1,250 in staff time recovered every single month — just from confirmation write-back alone.
Scale that across intake forms, demographic updates, and scheduling changes, and the efficiency gap between a clinical API and middleware scraping becomes a measurable budget line.
When you're comparing platforms, it's easy to evaluate what you can see — the interface, the feature list, the price. The architecture that sits underneath is harder to assess.
But it's also the variable that determines whether the platform actually reduces your staff's workload, or just adds a new tool to the stack that still requires manual follow-up to be useful.
The difference between curogram weave ehr integration architecture isn't a technical footnote. It's the practical question of whether your integration closes the loop on clinical data or leaves the last mile to your team.
The gap between displaying data and moving it is wider than it sounds. Every time your staff manually updates the EHR with information a patient already provided, that's time that didn't need to be spent that way.
It's also a margin for human error — a field not updated, a confirmation not logged, an intake detail missed.
These aren't small inefficiencies. They stack up into real operational cost.
Curogram's bi-directional API was built specifically to eliminate that gap for medical practices.
Not for dental offices. Not for veterinary clinics.
For the clinical data complexity that medical specialties actually operate with — medications, allergies, multi-condition histories, multi-provider scheduling, and real-time intake that needs to land in the right EHR field automatically.
Here's what that looks like in practice.
A mid-sized internal medicine group processes 800 appointment interactions per month. Before switching to a clinical API model, staff spent approximately 4 minutes per interaction on manual EHR updates — confirmation logging, intake transcription, demographic corrections.
That's 53+ hours per month. After implementing Curogram's bi-directional integration, those updates happen automatically. Staff hours shift from data entry to direct patient support.
And no-shows drop because EHR data is always current enough to power proactive outreach at the right moment.
That's not a hypothetical. It's the functional difference between a VoIP display layer and a clinical integration platform designed for the data demands of medical care.
Whether you're currently evaluating Weave, already using it and running into its limits, or looking at the full landscape of communication platforms for your practice — the architecture question is worth asking before you commit.
You're not just choosing features. You're choosing how deeply a platform connects to the record that drives your clinical and operational workflow every single day.
Schedule a Demo and see how a true clinical API changes what your team can actually stop doing.
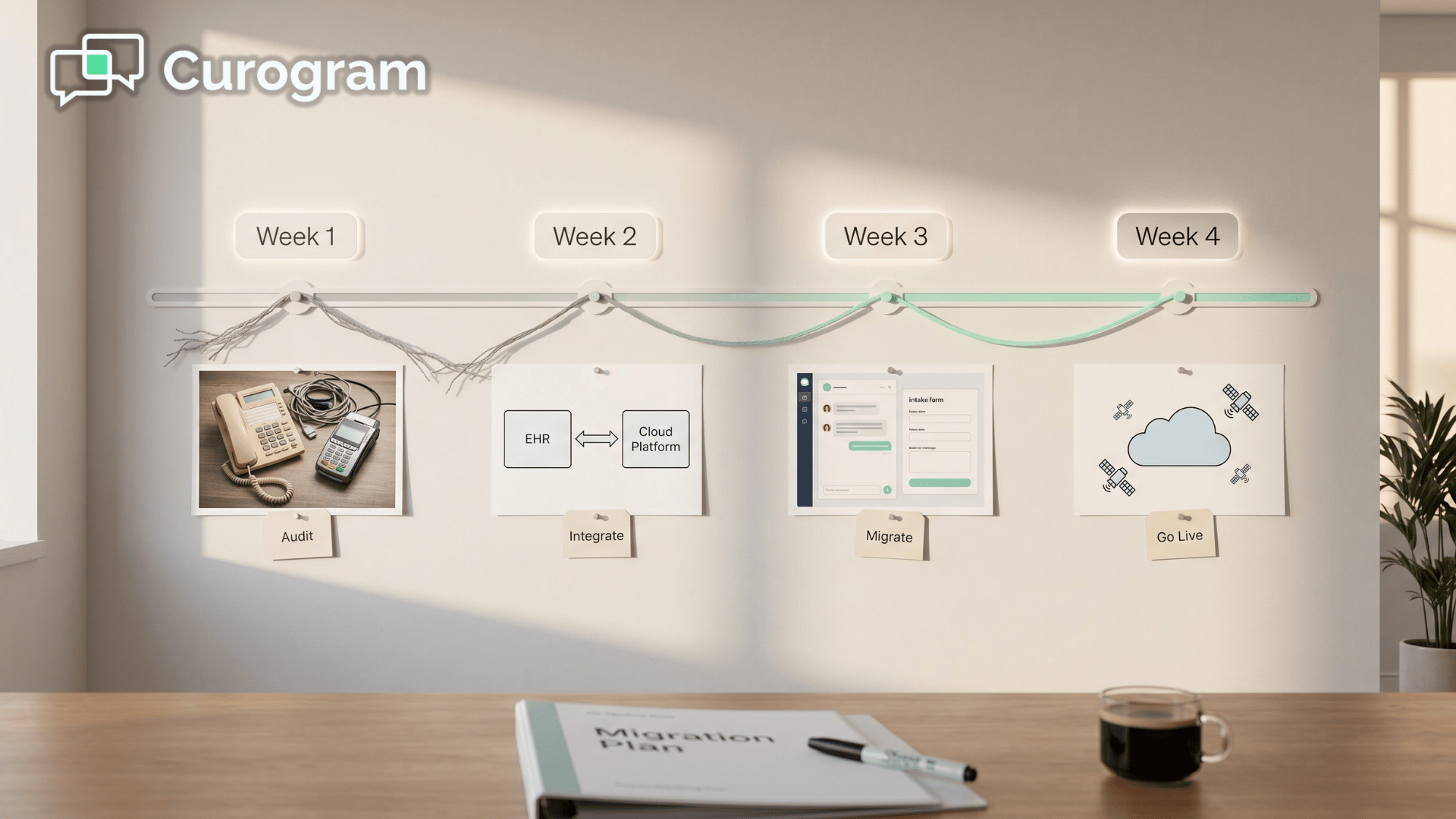
💡 A switch from Weave to Curogram migration moves your practice off VoIP-centric infrastructure and onto a medical-first clinical automation...
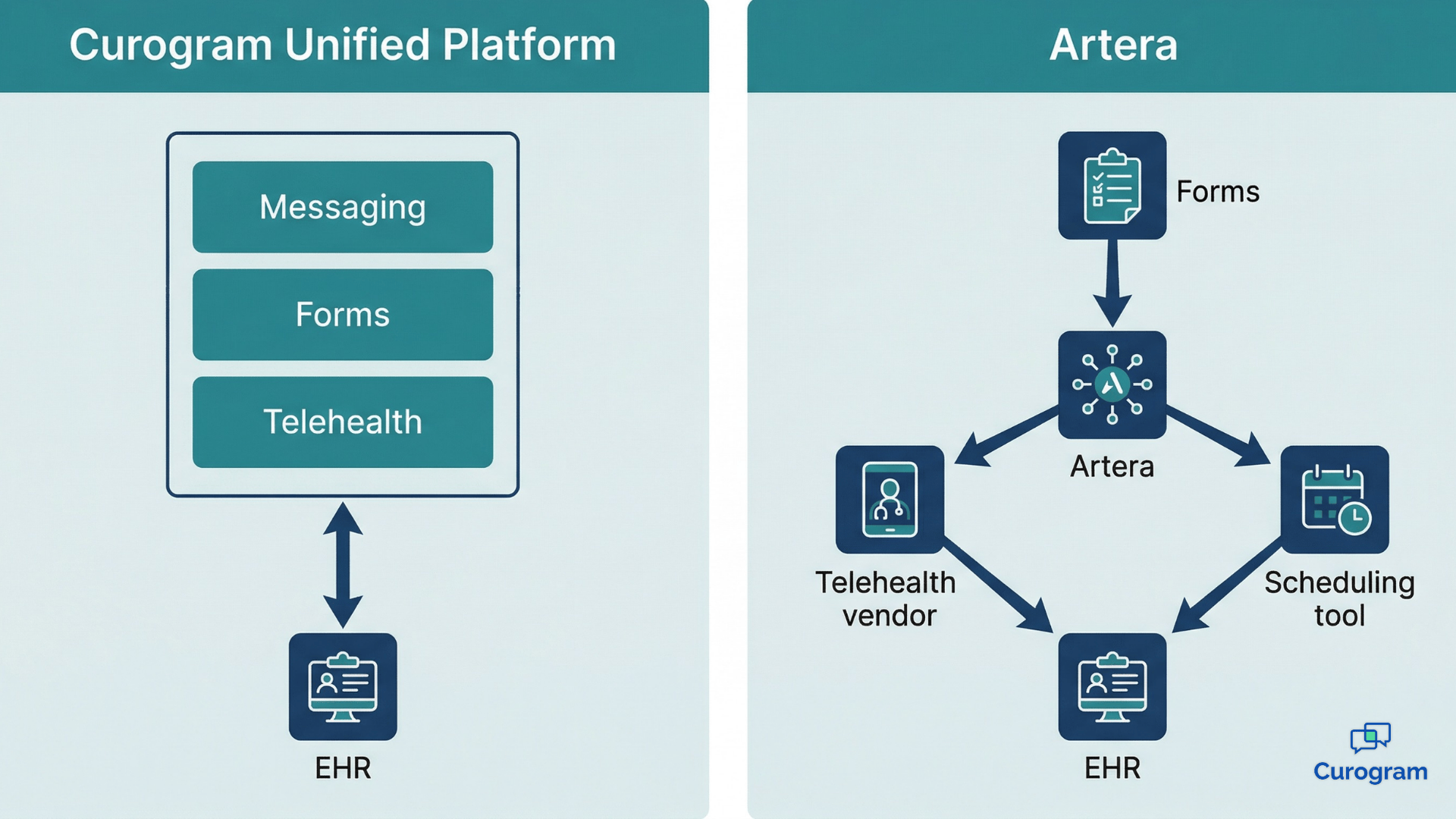
💡 When evaluating the Curogram Artera EHR integration architecture, the core difference is how each platform routes patient data to the record....
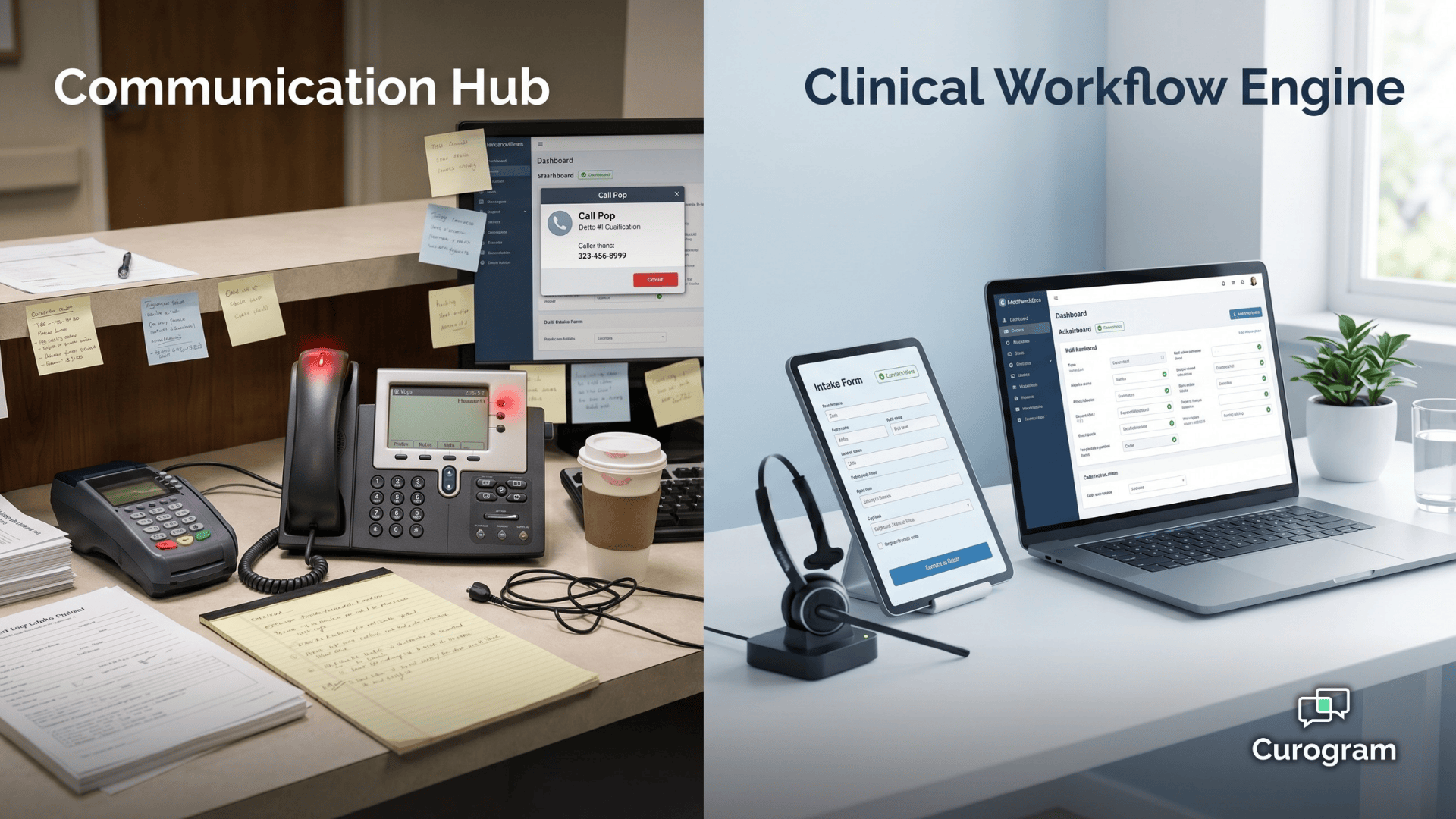
💡 Curogram and Weave take different paths to patient engagement. Curogram is built around clinical workflow automation, meaning confirmations,...