
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
Curogram vs. Artera: EHR Integration Architecture Compared
💡 When evaluating the Curogram Artera EHR integration architecture, the core difference is how each platform routes patient data to the record....
Think about this for a moment.
You made the decision to invest in a patient communication platform. On the surface, it looked like one system.
But the longer you used it, the more it revealed itself as something else — a hub connecting a form vendor, a telehealth vendor, a scheduling tool, and a reputation management system. Four contracts. Four renewal cycles.
Four separate points of failure. And one IT team trying to hold it all together.
It sounds like enterprise infrastructure. It works like a coordination problem.
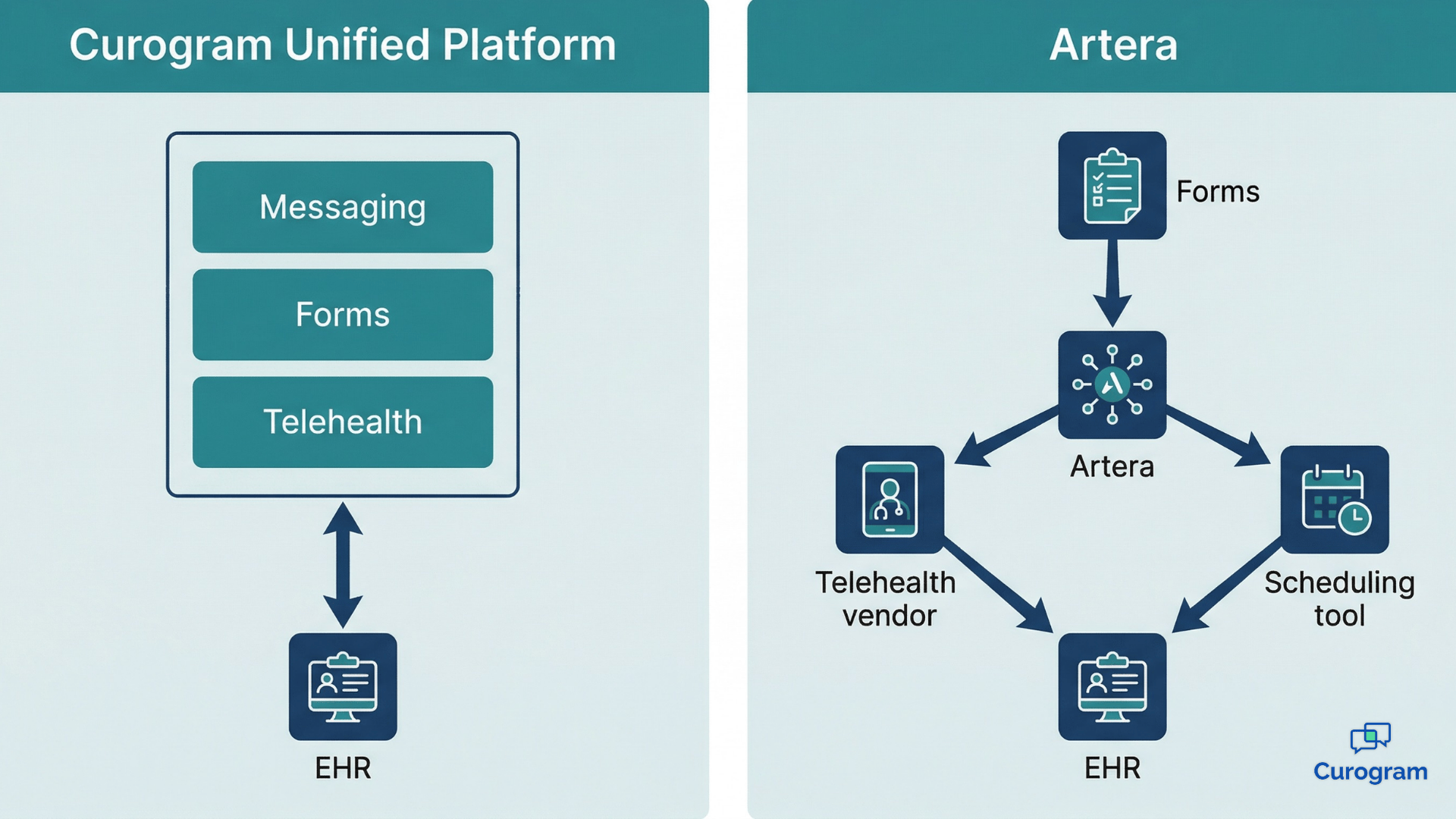
Health systems running Artera have described exactly this experience in verified industry reviews. Artera operates as a middleware orchestration hub — it routes messages and coordinates workflows across third-party vendors rather than natively performing those functions itself.
That architecture is manageable at small scale. Across dozens or hundreds of locations, it becomes a structural liability.
The cost compounds quietly.
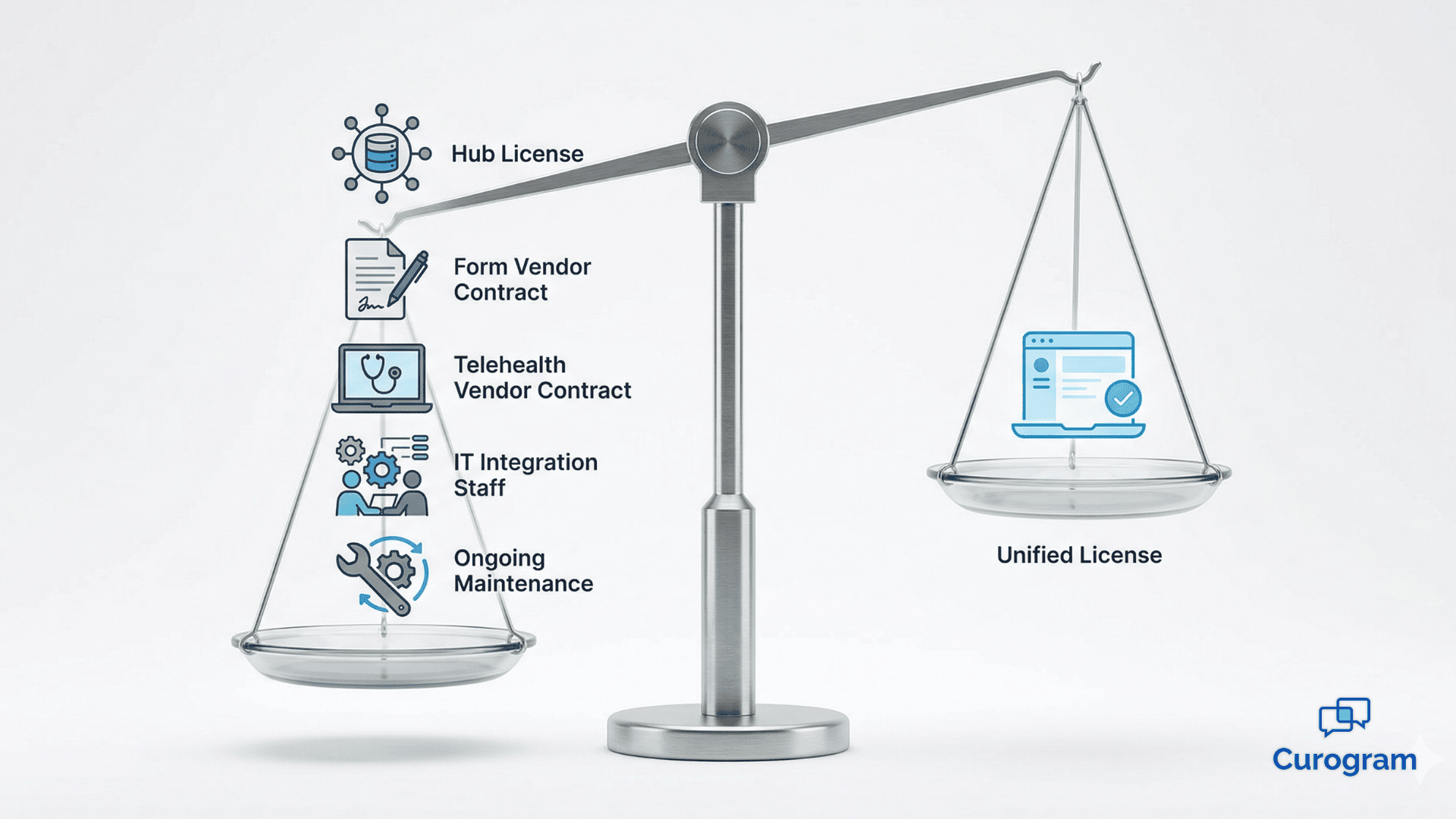
Vendor management overhead that multiplies with each new location. IT hours spent maintaining multi-point integrations. Staff trained on five different interfaces instead of one.
Separate contract negotiations, renewal timelines, and support escalations for every tool in the chain. None of these are dramatic line items on their own.
Together, they represent a platform that is more expensive to operate than it appears.
That's why health systems are now seriously evaluating what a switch from Artera to Curogram migration actually looks like in practice. Not as a feature-for-feature platform replacement.
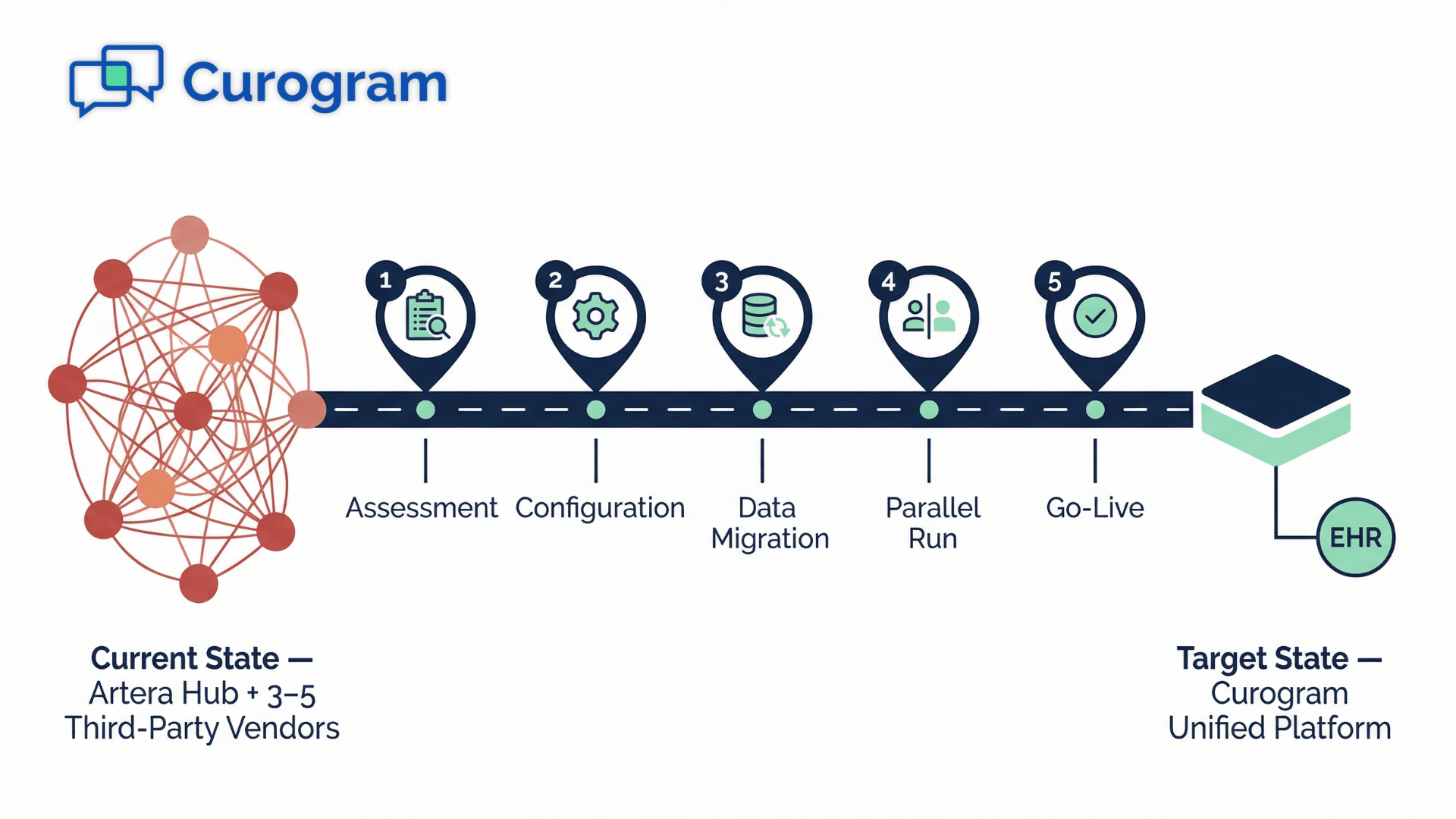
As a genuine healthcare vendor consolidation migration — folding three to five separate vendor relationships into a single, natively integrated clinical automation platform with one EHR connection and one team to call.
This article is the operational blueprint for that move. It covers the pre-migration audit, the implementation phases, the parallel-run strategy, and what your team should expect at every step of the way.
The migration is more manageable than your current stack makes it feel.
The decision to look for an artera alternative migration guide rarely happens overnight.
It builds over months of accumulating complexity — through support tickets that bounce between vendors, contract renewals that feel disproportionately hard to manage, and IT overhead that keeps growing even when the platform's core capabilities stay the same.
Artera's model is built around orchestration. Rather than natively delivering capabilities like intake, telehealth, or scheduling, Artera manages the flow of communication between separate third-party applications that do.
For organizations that started small, that model may have worked well enough.
For health systems managing large patient populations across many locations — some with 2.5 million patients across 172 sites — the model starts to work against them.
Verified industry reviews of the platform surface a consistent pattern: organizations cite escalating vendor management overhead, compounding integration maintenance costs, and the daily friction of coordinating multiple third-party tools behind a single messaging thread.
These aren't isolated complaints. They reflect what happens when orchestration architecture scales past the point where it can stay manageable.
This is precisely the operational environment that drives healthcare vendor consolidation migration conversations.
When the effort of managing the stack begins to outpace the value the stack delivers, health systems start looking for a structural change — not just a better vendor, but a fundamentally simpler architecture.
The complexity of a multi-vendor stack doesn't grow linearly — it compounds.
Add a new location, and you're not onboarding one platform. You're extending five.
Add a new service line, and each vendor has to be updated, retested, and re-integrated. One vendor's outage can disrupt the entire patient communication chain.
That's not a configuration problem. That's a design constraint built into middleware orchestration itself.
For health systems that have grown significantly or are planning to, this constraint becomes a ceiling. The question isn't whether the stack will create friction — it's how much friction the organization is willing to absorb before making a change.
Before any middleware to unified platform switch can begin, your team needs an honest and complete picture of what you're actually moving away from.
This means more than cataloging your Artera subscription. It means documenting every vendor that Artera orchestrates on your behalf, along with the workflows and data flows that depend on each one.
A thorough pre-migration assessment should inventory:
This inventory is not just administrative groundwork. It defines the real scope of the migration.
The common mistake health systems make is treating this as a one-to-one platform replacement. The actual scope is a vendor consolidation event — replacing three to five separate vendor relationships, integration endpoints, and training requirements with a single platform.
Understanding that distinction upfront changes how your team plans the budget, the timeline, and the change management process.
For health systems concerned about patient communication continuity during the transition — a legitimate concern when thousands of patients are receiving daily reminders, recalls, and telehealth links — the audit phase is also where you build your parallel-run strategy.
The goal of a parallel run is straightforward:
Activate Curogram alongside the existing Artera stack, validate automation performance in a live environment, and only decommission the legacy system once the new platform has demonstrated full operational effectiveness.
The audit tells you which workflows are most critical to validate first.
This phased approach significantly reduces the risk of disruption. Practices that plan the parallel run during the assessment phase — not after implementation starts — tend to reach go-live faster and with fewer unexpected gaps.

This is where the migration moves from planning into execution — and where the structural advantage of Curogram's architecture becomes immediately visible.
Curogram is not a middleware hub. It is a unified clinical automation platform, meaning the capabilities that Artera distributes across multiple third-party vendors are delivered by Curogram as native modules on a shared codebase, connected to a single EHR integration path.
That distinction changes the implementation process entirely.
Here is how the capability transition maps:
Every capability that previously required a separate vendor relationship is now delivered inside a single platform. That means one contract, one training requirement, one IT integration to maintain, and one support team to call when something needs attention.
The change in EHR integration architecture deserves particular attention, because it directly affects your IT team's workload long after the migration is complete.
In Artera's model, data often travels through a multi-hop path: from a third-party vendor, through the hub, through a translation layer, and then into the EHR. Each connection point is a potential failure surface and a maintenance responsibility.
Curogram replaces that entire chain with a single, direct bi-directional API connection between the platform and the EHR.
Your IT team goes from managing multiple integration endpoints — one per vendor, plus the hub itself — to maintaining one. That simplification doesn't just reduce workload during the migration. It reduces workload every day after go-live.
The implementation model isn't theoretical. Practices that have completed the patient communication platform transition to Curogram have documented concrete operational benchmarks.
Curogram deployments have achieved appointment confirmation rates above 75%.
No-show rates among implemented practices run 53% below industry averages.
To put that in practical terms: a mid-size practice handling 1,500 appointments per month with an average revenue of $200 per visit could conservatively recover $15,000 to $30,000 per month in previously lost appointment revenue, depending on their baseline no-show rate.
That's not a projection — it reflects what native automation performs like when it no longer depends on middleware to function.
For health systems evaluating the migration, these benchmarks represent the operational floor, not a ceiling.

To make the transition concrete, here is a direct comparison of what changes at each phase of the migration when moving from Artera's middleware orchestration model to Curogram's unified platform.
| Migration Phase | From Artera (Middleware Stack) | To Curogram (Unified Platform) |
|---|---|---|
| Vendor Contracts to Terminate | 3–5 (hub + form + telehealth + scheduling + reputation) | 0 — all capabilities are native |
| EHR Integration Points | Multiple — one per third-party vendor, plus the hub | 1 — single bi-directional API |
| Staff Retraining Scope | Multiple vendor interfaces to unlearn | Single platform to learn |
| Data Migration Complexity | Data distributed across hub and multiple vendors | Consolidated into one platform data layer |
| Parallel Run Feasibility | Complex — requires coordinating deactivation across vendors | Straightforward — single platform runs alongside legacy |
| Time to Full Automation | Dependent on remapping all vendor integrations | Rapid — native modules activate out-of-the-box |
| Post-Migration IT Overhead | Eliminated (no middleware mapping to maintain) | Lean — single integration path to maintain |
| Risk of Workflow Disruption | Higher — each vendor deactivation is a separate cut-over | Lower — unified platform replaces all functions simultaneously |
This table reveals a fundamental asymmetry.

In a middleware model, each phase of migration carries its own complexity because each vendor is a discrete deactivation event. In a unified platform model, the complexity is concentrated at the beginning — in the audit and configuration phase — and then simplifies dramatically at go-live and beyond.
For IT teams, the reduction from multiple EHR integration points to one is the most immediate structural improvement. Fewer endpoints means fewer maintenance obligations, fewer failure points, and faster troubleshooting when issues arise.
For operations teams, the reduction in staff retraining scope matters just as much. Training staff across five different vendor interfaces creates inconsistency, slower onboarding, and higher error rates.
A single platform with a unified workflow model is something staff can actually master.
For leadership, the vendor contract consolidation changes the financial picture.
Instead of negotiating five separate renewals — often on staggered timelines with different pricing models — you're managing one relationship. That simplification reduces administrative overhead and gives your organization significantly more leverage in pricing negotiations going forward.
At the end of this migration, you're not just running fewer vendor contracts. You're running a fundamentally different operational model.
That's the distinction worth sitting with. A middleware to unified platform switch isn't about trading one platform for another.
It's about removing a category of operational burden that most health systems have simply accepted as normal — the contract management, the multi-vendor IT maintenance, the staff training across five separate interfaces, the EHR integration troubleshooting that could originate from any one of three connection points.
None of those burdens are necessary. They are artifacts of an orchestration architecture that was never designed to simplify — it was designed to connect.
Curogram's unified model makes a different choice: to own the full clinical automation workflow natively, so nothing needs to be orchestrated across vendors at all.
For health systems managing significant patient volume and multiple locations, the financial math is clear. Eliminating three to five vendor contracts reduces direct technology spend. Recovering no-show revenue through native automation adds it back. Reducing IT maintenance hours frees your team for higher-value work.
And doing all of this on a single platform with a single EHR integration path gives you a technology foundation that scales cleanly rather than compounding in complexity.
The practices that have completed this migration aren't just saving money. They're running with fewer moving parts, less daily friction, and a platform that actually matches the operational complexity they were built to manage.
If your team is ready to map out what this migration would look like for your specific stack — your vendor count, your EHR environment, your locations — Curogram's implementation team can build that picture with you.
Schedule a demo to walk through the migration process, see the platform's native modules in action, and get a clear sense of what your timeline to go-live would realistically look like.
💡 When evaluating the Curogram Artera EHR integration architecture, the core difference is how each platform routes patient data to the record....
💡 Comparing Curogram and Artera on cost goes beyond subscription pricing. Artera's middleware orchestration model requires separate vendor...
💡 The difference between Curogram and Artera is operational. Curogram unifies patient messaging, intake forms, reminders, telehealth, recalls, and...