
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
NextGen Intake Forms | Structured Write-Back, Not PDF Attachments
💡 NextGen Enterprise patient intake forms built on Curogram's Structured Write-Back Pipeline deliver text-based forms to patients before their...
Think about what happens the moment a patient walks through your front door.
They hand over a clipboard, slide a form across the counter, or confirm they completed the portal intake.
Then your front desk staff — trained, experienced, expensive — sit down and start typing. Name. Date of birth. Insurance ID. Current medications. Medical history. Symptoms.
The same information the patient just wrote down, now entered again by someone else.
It sounds like a small thing. It isn't.
Across a 50-provider NextGen Enterprise network seeing 1,250 patients a day, that routine moment adds up to somewhere between 6,000 and 18,000 minutes of daily manual data entry.
That's staff time, payroll cost, and clinical capacity — all consumed by a task that produces zero clinical value. It simply moves data from one format to another.
This is what operations leaders inside large ambulatory organizations are starting to call the Transcription Tax. And it's hiding in plain sight, baked into every encounter, at every location, every single day.
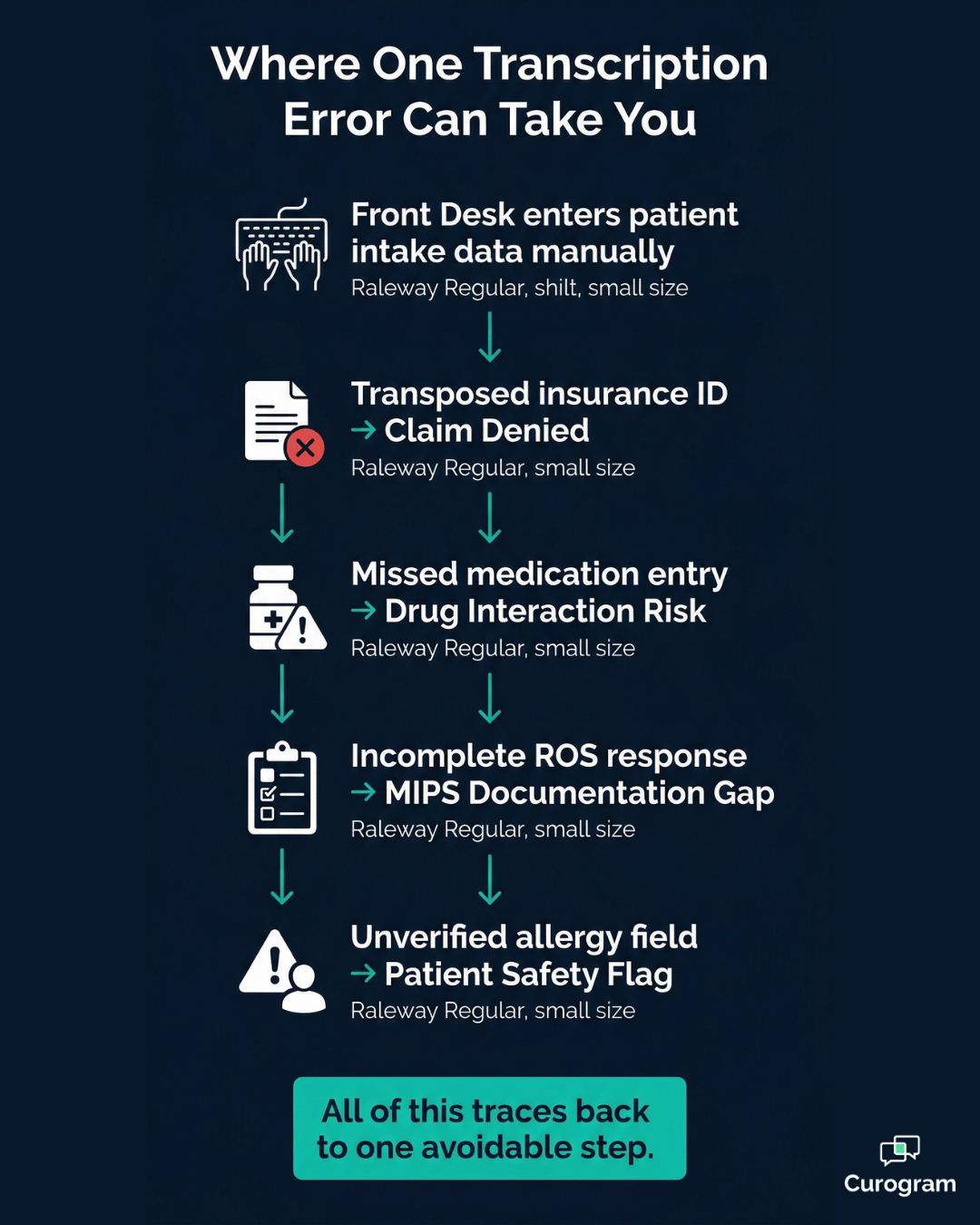
The problem runs deeper than wasted time. Manual entry creates transcription errors.
A miskeyed insurance member ID triggers a claim denial. A missed medication produces a drug interaction risk. An incomplete review of systems response creates a MIPS documentation gap.
At scale, these errors compound fast — and the consequences follow your revenue cycle and your compliance record long after the patient leaves.
And your front desk staff?
They know the redundancy is there. They know the patient already filled out the form. But without a direct bridge from what patients submit to what NextGen Enterprise needs, someone has to type it twice.
There is a better way. Curogram's approach to eliminating NextGen front desk intake transcription — a structured write-back workflow called Zero-Entry Check-In — automates the entire pipeline from patient form submission to chart population.
No manual entry. No bottleneck. No errors introduced by a second pair of hands.
Here's how it works, and why it changes everything downstream.
Walk into any high-volume NextGen Enterprise location during morning check-in, and you'll see the same scene. A patient completes an intake form — paper, PDF, or portal — and hands it to the front desk.
The staff member opens NextGen Enterprise and starts typing. Field by field. Screen by screen.
For a straightforward primary care visit, that process takes 5 to 7 minutes.
For a complex specialty intake — orthopedic surgical history, behavioral health screening, cardiology risk assessment — it takes 10 to 15 minutes.
Multiply that by 25 patients per provider per day, across 50 providers, and the numbers become hard to ignore.
That's potentially 18,750 minutes of daily transcription labor across the network. Spread across a five-day week, it works out to roughly 375,000 minutes per month — or the equivalent of over 1,000 eight-hour shifts dedicated entirely to retyping what patients already wrote.
For your revenue cycle team, the number that matters most isn't time. It's errors. One transcription mistake per 20 patients means 62 or more errors per day across a 50-provider network.
Here's where those errors land:
Each one is traceable back to a manual reentry step that was never necessary in the first place. At enterprise scale, these aren't edge cases. They're a predictable, recurring cost of keeping intake manual.
The transcription step doesn't just cost time. It creates a constraint that backs up the entire visit workflow.
When intake data entry sits between patient arrival and chart readiness, the clinician can't begin the encounter. The room can't be prepped. And at high-volume locations processing 200 or more patients per day, that delay cascades.
Morning check-in delays push rooming back. Rooming delays push encounters back. By mid-afternoon, the schedule is running late — and the cause traces back to a single slow step no one has fully addressed.
The intake process should be the fastest, most automated step in the visit. Instead, it's often the constraint.
Front desk staff at many NextGen Enterprise locations spend 30 to 50% of their shifts on intake data entry.
That's half their workday dedicated to a task a computer could handle. Staff who should be managing patient flow, coordinating referrals, and answering complex inquiries are instead copying data from a form into a screen.
The redundancy is obvious to everyone doing it. The frustration is real. And the turnover risk that comes with high-volume, low-value manual work isn't abstract — it shows up in your hiring costs and your onboarding calendar.
Eliminating PDF transcription for NextGen intake forms isn't just an efficiency play. It's a staff retention conversation.
Curogram's Zero-Entry Check-In reengineers the intake pipeline from the ground up.
The goal is simple:
Take what the patient submits and route it directly to the structured chart fields in NextGen Enterprise — without staff touching the data in between.
Here's how the workflow runs:
Zero staff data entry. Zero bottleneck. Zero errors from a second set of hands.
This is structured write-back — not a PDF attachment, not a scanned form, and not a workaround. Each field maps directly to the correct structured location in NextGen Enterprise.
The bigger operational shift isn't just about removing a task. It's about when intake happens.
Under the traditional model, intake happens at arrival: the patient walks in, completes a form, and staff transcribes the data while the patient waits. Under Zero-Entry Check-In, intake is completed before the visit. The chart is pre-populated by the time the patient walks through the door.
That changes what check-in actually means. Instead of data collection, it becomes data verification.
Staff ask:
"Is your address still 123 Main Street? Is your insurance still the same?"
That conversation takes 60 seconds, not 10 minutes.
For high-volume locations processing 200-plus patients daily, that shift eliminates the primary source of morning check-in delay.
Structured write-back runs via API-based integration with NextGen Enterprise.
IT directors can review the field-level mapping for each form template and verify that data writes to the correct chart fields before go-live. Every write-back is logged, encrypted, and compliant with SOC 2 Type II and HIPAA requirements.
The integration is also independent of NextGen's desktop performance. Intake data flows to the chart even when NextGen's screens are running slow — which matters in high-volume environments where system lag is a real operational factor.
This is where the enterprise fit becomes clearer. Zero-Entry Check-In adapts to how each location and specialty operates, without requiring rigid uniformity across the network.
Each specialty type gets its own form and mapping configuration:
Each location's configuration is fully independent. Changes at one site don't affect another, and form templates can be updated without touching the mapping logic at other locations.
For NextGen multi-location intake automation, this kind of configuration flexibility is what makes network-wide deployment viable.
Consistent data quality across dozens of locations, without sacrificing the specialty-specific workflows each team depends on.

Text-delivered intake forms achieve completion rates above 80% before the visit. That means more than 4 out of 5 charts are pre-populated before the patient walks in.
For a 50-provider network, that translates to 1,000 or more patients arriving with fully structured chart data already in place — each day.
Eliminating 5 to 15 minutes of manual transcription per patient recovers between 6,000 and 18,000 staff minutes daily across that same network. That's the equivalent of 8 to 25 full-time employees no longer spending their days on manual data entry. In practice, this means your existing staff have capacity for work that actually moves the operation forward.
Here's what that looks like as a monthly estimate:
| Scenario | Daily Transcription Time Saved | Monthly Staff Hours Recovered |
|---|---|---|
| 50 providers, 5 min/patient avg | 6,250 min | ~521 hours |
| 50 providers, 10 min/patient avg | 12,500 min | ~1,042 hours |
| 50 providers, 15 min/patient avg | 18,750 min | ~1,563 hours |
At a burdened front desk labor cost of $25 per hour, the mid-range scenario alone represents over $26,000 in recovered labor value every month.
That's not a projection — that's staff time redirected to patient-facing work your organization is already paying for.
The role of your front desk staff doesn't disappear — it gets better.
Instead of typing demographics from a PDF, they confirm: "Is your information still current?"
The check-in conversation becomes a 60-second verification step instead of a 10-minute data collection process. Staff capacity opens up for managing patient flow, processing referrals, and handling the complex inquiries that actually require human judgment.
The bottleneck that backed up your waiting room disappears because the slowest step in the patient check-in workflow has been automated. And for your clinical staff, the change is equally significant.
Charts arrive pre-populated with structured data before the encounter starts — which means less documentation time during the visit and less after-hours charting when the day is done.
When NextGen clinical staff intake data quality improves through automated structured fields, every team across the organization feels the difference — but in different ways:
This is what a fully automated intake pipeline looks like at the enterprise level.
Not a workaround. Not a portal that still requires staff to reconcile the output. A direct, structured, field-level connection between what the patient submits and what NextGen Enterprise requires.
There's a cost you've been absorbing for years without naming it.
It sits inside every patient encounter, at every location, on every shift.
It's the gap between what patients submit and what NextGen Enterprise needs — filled manually, every time, by front desk staff who should be doing something else entirely.
The math is straightforward. Across a 50-provider network, 10 minutes of manual transcription per patient adds up to more than 1,000 recovered staff hours per month at the mid-range estimate.
That's real capacity — not headcount reduction, but redeployment toward the patient-facing, revenue-generating work your team was hired to do.
Curogram's Zero-Entry Check-In closes that gap. The patient fills out a form on their phone before the visit. The data flows directly into NextGen Enterprise's structured chart fields. By the time the patient walks in, check-in is a 60-second confirmation conversation — not a 10-minute data collection exercise.
No manual entry. No transcription errors. No waiting room backup.
For VP-level operations leaders and COOs managing multi-specialty NextGen Enterprise networks, this is the kind of change that shows up in throughput metrics within the first month.
Front desk supervisors see it in their daily workflow. Clinicians see it in pre-populated charts. Revenue cycle teams see it in cleaner claim submissions. And your front desk staff — the ones who've been typing demographics into screens for years — finally have the capacity to do the work that actually requires them.
NextGen Enterprise is where your clinical data lives. Curogram is how it gets there — without staff typing it twice.
Schedule a demo today. Bring your KBM templates and your specialty configurations.
💡 NextGen Enterprise patient intake forms built on Curogram's Structured Write-Back Pipeline deliver text-based forms to patients before their...
💡 Curogram’s “Two-Minute Intake” texts patients a form before their visit. They complete it on their phone, and the data writes directly into...

💡 Rural patient pre-registration via text for Azalea Health clinics lets patients complete their intake forms at home — before they ever walk...