
 Jo Galvez
Jo Galvez
Digital Intake for Exa PACS | Safety Screening Automation
💡 Paper intake forms slow down imaging centers in three ways. They create waiting room delays, introduce safety blind spots, and require manual...
Think about the last time a patient sat in your waiting room, still filling out forms just minutes before their MRI. That small moment costs more than just time.
Radiology intake is not like a routine checkup. Before a patient enters a scan room, your team must verify their full safety history. Metal implants, contrast allergies, and pregnancy status are not minor details. They are clinical requirements that keep patients safe.
Most imaging centers still handle this on paper or with in-office tablets. Patients arrive and start writing. Your schedule slips, studies back up, and your staff re-types handwritten answers into Exa RIS. Across 20 patients a day, that adds up to hours of wasted clinical time.
This is not just slow. It is a real safety risk.
Exa RIS manages your images, studies, and patient records with precision. But it does not reach patients before they walk through your door. That gap is where delays build, safety disclosures get missed, and revenue quietly slips away.
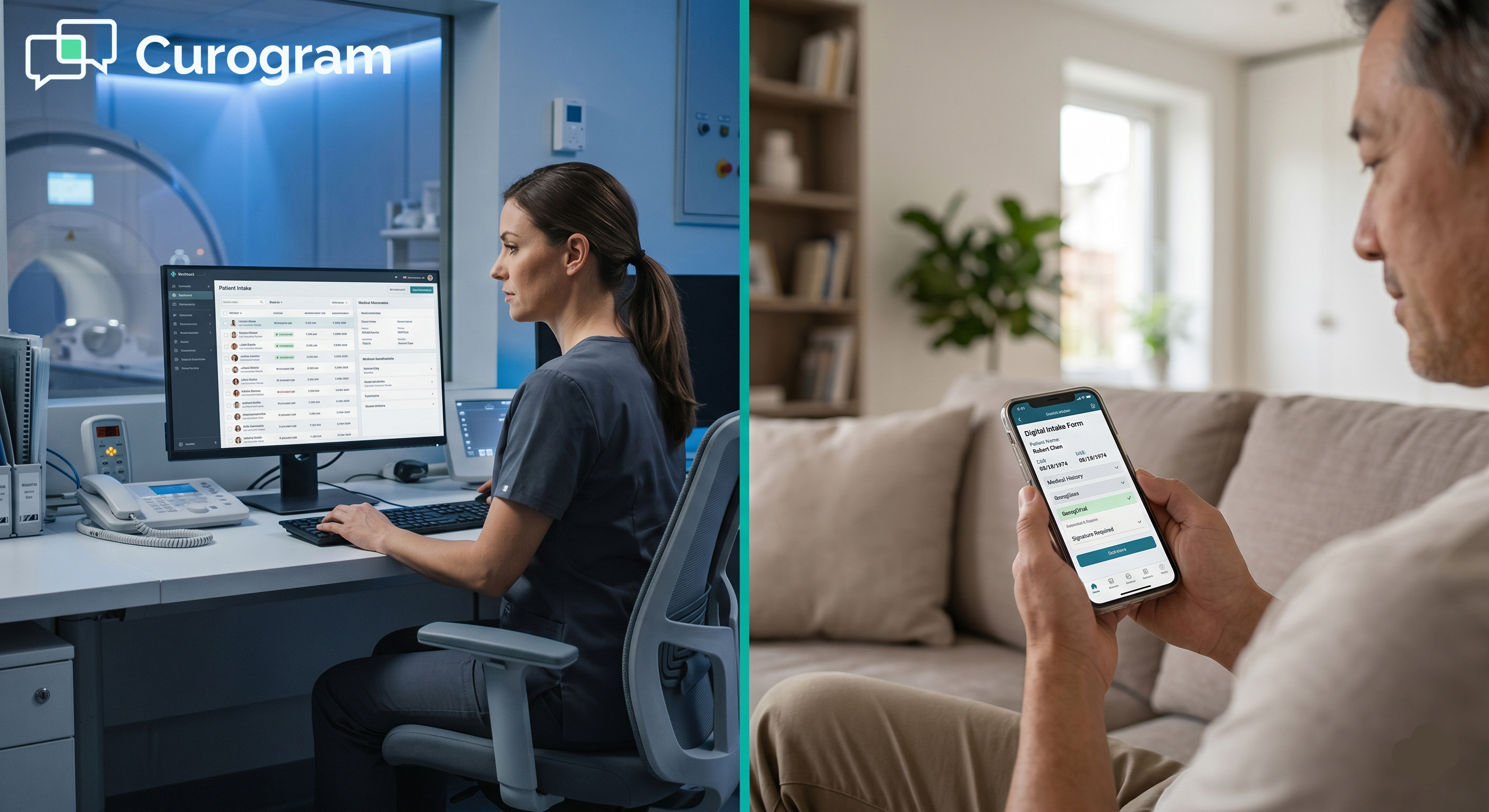
Curogram bridges that gap. It sends secure online forms to patients 24 to 48 hours before their visit via text message. Patients complete their forms at home, on any device, with no app or portal login required.
By the time your first patient arrives, their MRI safety screening is already done. The data is in Exa RIS. Your tech has everything they need. Your radiologist has reviewed any flags, and the scan starts on time.
This is what radiology digital intake looks like when it works. Not a clipboard. Not re-entered data. Not a delayed study.
In this guide, we cover why paper intake puts your center at risk, how pre-arrival text forms change that, and what real results look like in practice.
Paper-based intake might seem like a small issue. But in a radiology center, it creates a chain of problems that touches safety, daily operations, and your bottom line. Let us walk through what that actually looks like.
Radiology intake is a safety function above everything else. Collecting safety data minutes before a scan leaves almost no time for review or follow-up. That tight timeline puts both patients and your team in a difficult position.
Handwritten forms are full of gaps. Patients skip fields, pick the wrong box, or write answers that are hard to read. Staff try to make sense of responses under time pressure. When something is unclear, they often move on to the next task.
In radiology, a missed field is not a minor clerical error. It is a potential safety incident. The ACR MRI safety guidelines require complete, verified screening before any patient enters the scan room. Paper forms make that standard hard to meet every time.
Even a correctly filled paper form creates a timing problem. Your tech gets the form moments before the patient heads into the scan room. There is no buffer to call a physician, check with the radiologist, or adjust the protocol.
This is the window where things go wrong. A contrast allergy that needs a protocol change. A pacemaker that rules out the MRI entirely. Catching these issues after the patient is already in your facility creates confusion, delays, and serious safety exposure.
The safety risks are real. But there is also a direct financial cost tied to on-site intake that many imaging centers overlook. The math is simpler than it looks.
On-site intake typically takes 15 to 30 minutes per patient. That includes filling out forms, handing them to staff, manual data entry into Exa RIS, and any follow-up questions. In a center that scans 20 patients per day, that adds up to 5 to 10 hours of clinical time spent on intake alone.
Over a full working week, that adds up to a full day of clinical capacity lost to paperwork. Your scan rooms sit idle while your techs do data entry instead of running studies.
The table below shows the key differences between paper-based and text-based digital intake:
|
Factor |
Paper / On-Site |
Curogram Text-Based |
|
When intake happens |
On arrival |
24 to 48 hours before arrival |
|
Time per patient on-site |
15 to 30 minutes |
Near 0 minutes |
|
Data entry |
Manual re-entry into Exa RIS |
Auto-syncs directly to Exa RIS |
|
Safety flag review |
Minutes before the scan |
Hours before the patient arrives |
|
Pre-arrival completion rate |
0% |
70 to 85% |
Every delayed scan is a missed chance to book another study. If intake pushes your schedule back by 15 minutes per patient, the ripple effect compounds fast. Based on our internal data, imaging centers that move to pre-arrival digital intake recover an average of 2 to 4 extra studies per day.
At a typical study value of $500 to $2,000, that is meaningful, recurring revenue. And it does not require hiring more staff or extending hours. It just requires moving intake out of your waiting room and into the patient's hands the night before.

A text message might seem too simple to fix a clinical workflow problem. But the simplicity is exactly what makes it work. Here is how the process unfolds, from the patient's phone to your Exa RIS records.
Curogram sends a secure intake link to the patient's phone 24 to 48 hours before their appointment. The patient taps the link on any device and fills out their forms. No app download is required. No portal account. No printed instructions to follow.
Every part of the process is HIPAA compliant. The text message itself carries no protected health information. The form is delivered through an HTTPS-encrypted link. Every submission, edit, and view is logged for your audit trail.
The patient experience is designed to reduce friction. They receive a text, tap the link, and fill out their form. Most patients finish in 10 to 15 minutes. Based on our internal data, 70 to 85% of patients complete their forms within four hours of receiving the link.
That means your morning starts with most intake already finished. Your front desk is not chasing down paperwork. Your radiologist is not reviewing safety data with one eye on the clock.
Some forms are routine. Others contain responses that need immediate clinical attention. Curogram handles both cases without extra effort from your team.
When a patient flags a metallic implant, a contrast allergy, or a pregnancy, the system sends an instant alert to your radiologist or clinical coordinator.
This notification goes out hours before the patient is scheduled to arrive. That gives your team time to adjust the protocol, follow up, or reschedule safely.
Collecting the data is just the first step. What matters is where that data ends up and how fast it gets there. The Curogram integration with Exa RIS ensures your team never has to re-enter a form response by hand.
Curogram connects to Exa RIS through a REST API. When a patient submits their form, the response data flows directly into their Exa RIS patient record. Allergies, safety flags, and consent signatures all appear in your workflow without manual input from your team.
This removes one of the most common error sources in radiology: transcription mistakes. When data moves automatically from the patient to Exa RIS, your team spends less time entering data and more time reviewing it. That is a safer, faster, and more accurate use of clinical resources.
One intake template does not fit every scan type. An MRI safety questionnaire covers metal implants, implanted devices, and claustrophobia. A CT contrast screening form focuses on allergy history and kidney function.
Mammography requires symptom history and consent. Curogram lets you build and route the right form based on appointment type.
The table below shows the key form requirements for each common scan type:
|
Scan Type |
Key Form Requirements |
|
MRI |
Metal implant history, implanted devices, claustrophobia history, safety consent |
|
CT (with contrast) |
Allergy history, kidney function assessment, contrast media consent |
|
Mammography |
Symptom history, prior imaging records, consent form |
|
Ultrasound |
Prep confirmation, symptom notes, order verification |
Your scheduling system triggers the correct form for each scan. The patient never sees the wrong questions. Your team never reviews the wrong intake form.
Moving intake out of the waiting room creates measurable improvements in daily operations. These are not projected gains. They are outcomes that imaging centers see in the first weeks after switching to pre-arrival digital forms.
The key metric to watch is pre-arrival completion rate. With paper forms handed out at the desk, that number is effectively zero. Patients fill them out on arrival, not before.
With text-delivered forms, that number jumps to 70 to 85%. That single change reshapes how your entire day operates, from your first appointment to your last.
Patient portals have a well-known engagement problem. They require account creation, password management, and multiple steps before a patient reaches their form. Many patients simply do not use them, especially for a one-time imaging visit.
Text messages are different. Most people open a text within minutes. There is no login, no forgotten password, and no app to install. The patient taps a link and fills out their form on a device they already use every day. That simplicity is why text-based digital intake reaches completion rates that portal-based systems rarely match.
Picture a center scanning 20 patients per day. At 70% pre-arrival completion, 14 patients arrive with their intake already done. Your staff handles on-site forms for only 6 patients instead of 20. That cuts your morning intake load by 70%.
At 85%, 17 patients arrive ready to scan. Your team manages only 3 on-site forms. Your schedule starts on time. Your scan rooms run at full capacity from the first appointment of the day.
Pre-arrival digital intake does not just reduce paperwork. It gives back time that used to be lost to on-site processing. That recovered time translates directly into scan capacity and additional daily revenue.
If 15 out of 20 patients complete intake before arrival, your center recovers 3 to 7 hours of clinical time each day. Your techs are scanning instead of waiting on forms. Your scan rooms are running instead of sitting idle.
That recovered time does not disappear into overhead. It converts directly into additional scan capacity, and more capacity means more studies.
Based on our internal data, imaging centers that adopt pre-arrival digital intake recover an average of 2 to 4 extra studies per day. At a study value of $500 to $2,000, the impact adds up quickly.
The table below estimates revenue gains at different recovery scenarios, based on 250 operating days per year:
|
Studies Recovered / Day |
Avg. Study Value |
Daily Revenue Gain |
Annual Estimate* |
|
2 studies / day |
$500 |
$1,000 |
$250,000 |
|
3 studies / day |
$1,000 |
$3,000 |
$750,000 |
|
4 studies / day |
$2,000 |
$8,000 |
$2,000,000 |
*Based on 250 operating days per year. Actual results will vary by center volume and study mix.

Your Exa RIS system is built for precision. It stores your images, tracks your studies, and keeps your patient records in order. But the clinical workflow starts the day before, when a simple text message asks patients to complete their intake from home.
When that step is missing, everything else is harder. Safety reviews are rushed. Data is re-entered by hand. Flags go unnoticed until the patient is already in your facility, and your schedule pays the price.
Pre-arrival digital intake is both a safety upgrade and a revenue recovery tool. The table below summarizes what Curogram adds to your Exa RIS workflow:
|
Challenge |
What Curogram Does |
|
Paper forms and on-site delays |
Sends intake forms via text 24 to 48 hours before the visit |
|
Missed or illegible safety data |
Collects verified responses before the patient arrives |
|
Manual data re-entry |
Syncs form data directly into Exa RIS |
|
Rushed safety flag review |
Sends conditional alerts hours before the patient arrives |
|
Low intake completion rates |
Achieves 70 to 85% pre-arrival completion |
Radiology intake is not just about forms before a scan. It is how your team confirms the procedure is safe to perform.
When that process happens in the waiting room, minutes before scanning begins, you are collecting safety data too late to act on it. Moving that step 24 to 48 hours earlier changes the entire risk profile.
Earlier intake gives your team time to respond to safety concerns before they become on-site problems. A contrast allergy caught the day before is a simple protocol change.
Caught on-site, it disrupts your full schedule and puts the patient at risk. Pre-arrival forms close that gap consistently, across every patient.
Curogram logs every form submission, response, and access event automatically. There is no extra work from your team to maintain this record. Your audit trail meets HIPAA and state regulatory standards. Every patient's safety history is fully documented before the first scan of the day begins.
When intake takes 15 to 30 minutes per patient on-site, that time comes directly out of your scan schedule. Recovering it through pre-arrival forms is one of the most direct ways to increase daily study volume and daily revenue.
Based on our internal data, imaging centers that switch to pre-arrival digital intake recover an average of 2 to 4 extra studies per day. Over a full year, at a typical study value of $500 to $2,000, the cumulative revenue gain can reach hundreds of thousands of dollars. No added staff. No extended hours. Just a smarter intake process, easier appointment, and faster payment.
Curogram integrates with Exa RIS in hours, not weeks. There is no lengthy IT project and no hardware to install. Most centers see measurable gains in intake completion within their first week.
Schedule a free demo and see how many empty imaging slots you can fill.

💡 Paper intake forms slow down imaging centers in three ways. They create waiting room delays, introduce safety blind spots, and require manual...

💡 MRI safety intake forms protect patients. But filling one out in a cold waiting room — rushed and confused — leads to missed details and wrong...

💡 Small Office Ally practices lose 10 to 15 minutes per new patient to clipboard check-in. Staff print forms, hand out pens, collect pages, and...