
 Aubreigh Lee Daculug
Aubreigh Lee Daculug
Digital Patient Intake for Osmind | Pre-Treatment Screening via SMS
💡 Digital pre-treatment screening forms Osmind interventional psychiatry SMS workflows let you send PHQ-9, GAD-7, and safety assessments through a...

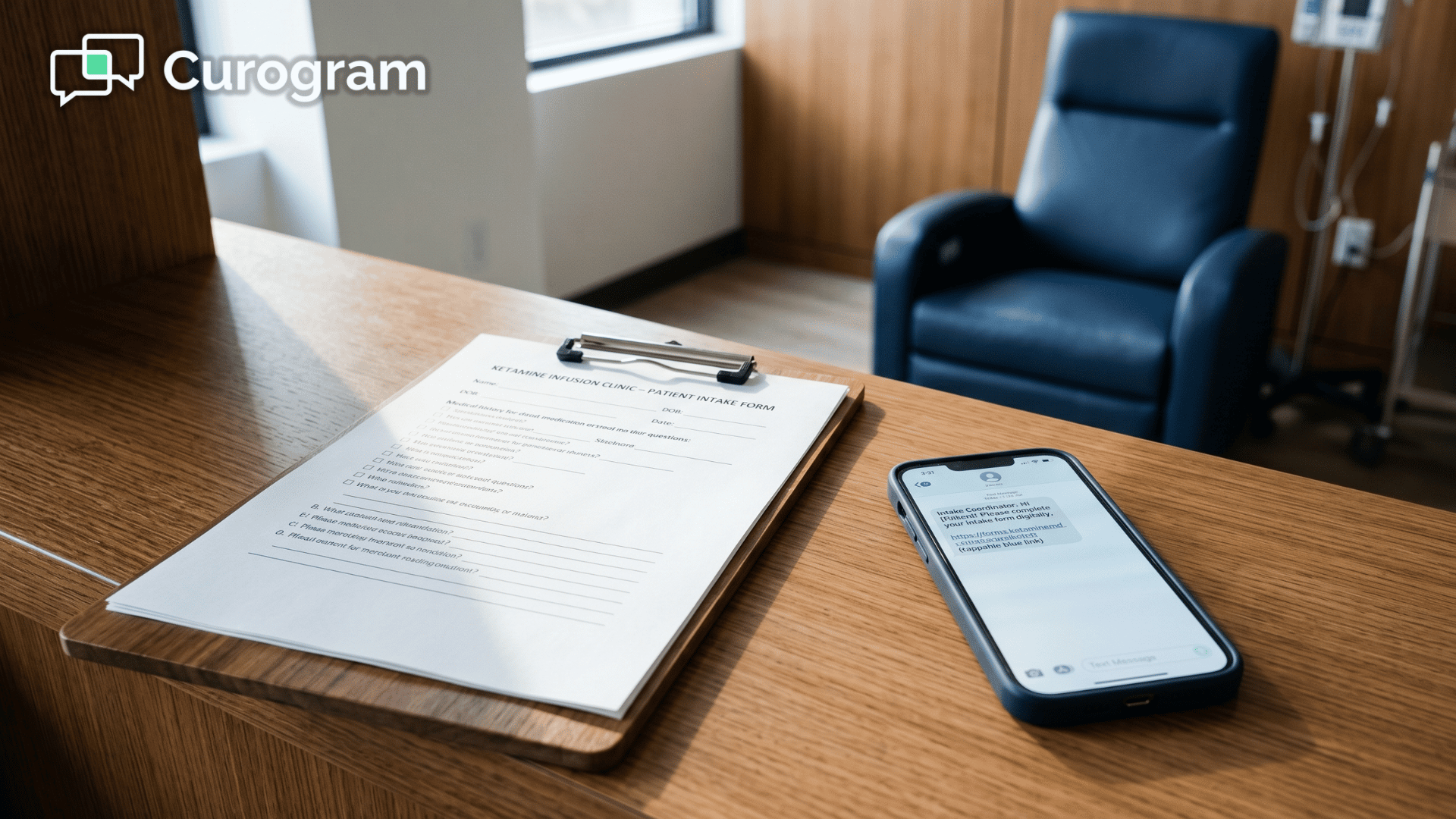
A patient walks into your clinic for a ketamine infusion. They are handed a clipboard. On that clipboard is the PHQ-9. Question 9 asks about thoughts of being better off dead or hurting themselves.
They look up. The waiting room is half-full. The front desk is three feet away. They check the box that says "Not at all."
It is not true. They have had those thoughts for months. That is why they are sitting in your clinic in the first place.
This is the quiet failure of clipboard screening in interventional psychiatry. The questions are sound. The clinical intent is right. But the setting works against honesty.
Sensitive screenings only do their job when patients feel safe answering them. A waiting room full of strangers is not that setting. Neither is a clipboard that gets handed back to a receptionist.
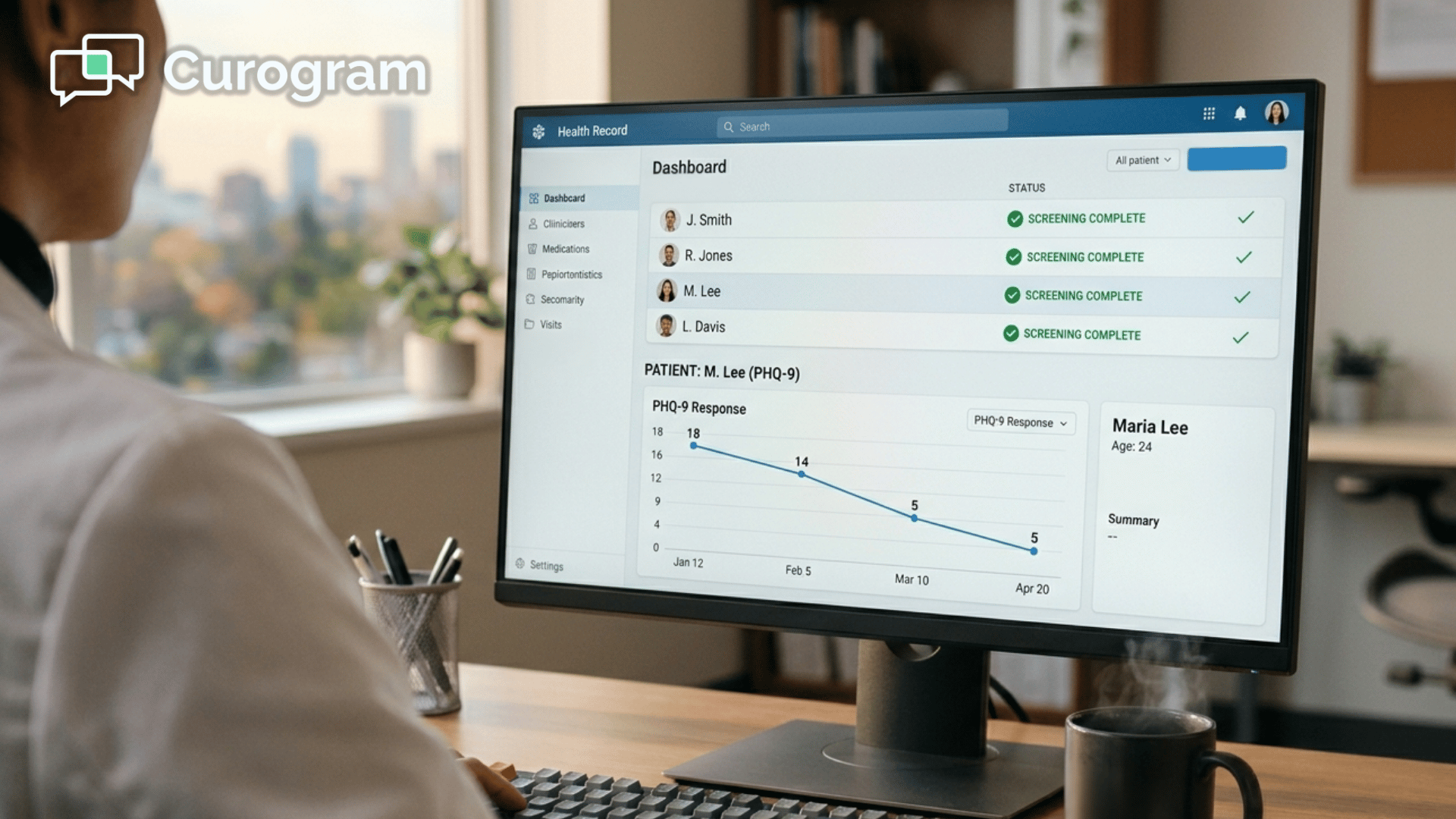
For practices running on Osmind, this matters in a specific way. Osmind's measurement-based care tools are built around clean longitudinal data. PHQ-9 trends. C-SSRS responses. Treatment-response curves over weeks and months. Every flag, every plotted point, every AI-surfaced pattern depends on patients telling the truth at the start.
If they soften their answers in the waiting room, your data is soft too. You are not tracking their real condition. You are tracking what they were willing to say in public.
There is a better way to do this, and it does not require an app, a portal login, or a new EMR. It requires moving the screening out of the waiting room and into the patient's home, where privacy supports honesty.
That is what this article is about: at-home pre-treatment screening Osmind patients private SMS form completion, and why it produces better clinical data for your team.
Interventional psychiatry asks patients to disclose the most sensitive parts of their lives on paper. The C-SSRS asks directly about suicidal thoughts, plans, and intent. The PHQ-9 asks about hopelessness and self-harm. Safety checklists ask about recent substance use, medication changes, and psychological state in the past 48 hours.
These are not routine intake questions. They are clinical disclosures. They require trust, privacy, and the absence of social pressure.
A waiting room offers none of those things.
Your patient checks in for their infusion. A staff member hands them a clipboard. They sit down and start working through the form,
But the room is working against them in small ways they barely notice:
They scan question 9 of the PHQ-9. They have had those thoughts. They mark "Not at all." They scan a substance use question. They had a glass of wine last night. They check "No." The screening proceeds, the form gets handed back, and the infusion happens on incomplete information.
Inside Osmind, that PHQ-9 score becomes a data point. It plots on a trend line. It feeds into outcome tracking and may surface in pattern reports later. If the patient softened five questions out of nine, the score is artificially low.
A baseline that is 4–6 points below reality skews every follow-up reading after it. You may think the patient is responding to treatment when they are simply reporting the same softened answer every visit.
This is what private patient screening interventional psychiatry Osmind is meant to fix. Not the form itself. The environment around the form.
Underreporting is not just a data hygiene problem. It is a safety problem. When patients soften answers on a clipboard,
The suppression usually shows up in the same few places:
If a patient minimizes suicidal ideation on a pre-infusion screening, your clinical team may not raise monitoring intensity for that day.
If they minimize substance use, the infusion proceeds without complete safety information. The screening exists to surface risk, and a clipboard in a busy room actively suppresses that signal.
Published research in journals like JAMA Psychiatry and the Journal of Medical Internet Research has consistently shown that patients disclose sensitive symptoms at higher rates when assessments are private and technology-mediated, compared to paper completed in clinical settings.
Below is a sample scenario for one practice running 200 pre-infusion screenings per month.
The numbers are illustrative, not promised outcomes.
| Screening Setting | Estimated Honest Disclosure on Q9 (PHQ-9) | Flags Surfaced per Month | Flags Missed per Month |
|---|---|---|---|
| Clipboard in waiting room | ~60% | 12 of 20 expected | 8 |
| Private SMS form at home | ~90% | 18 of 20 expected | 2 |
| Net difference | +30% | +6 flags caught | 6 fewer missed |
If even 6 additional safety flags per month reach your clinical team before the patient walks in, that is 6 opportunities to adjust monitoring, modify the conversation, or pause treatment.
Across a year, that is 72 patients whose risk was visible to you in advance instead of buried under social pressure.
For your team, this means safer infusions. For your data, it means PHQ-9 completion at home text link Osmind produces a cleaner curve than clipboard data ever will.
Most practices already know clipboard screening is imperfect. The fixes that usually get tried sound reasonable on paper but break down in practice.
Pre-infusion assessment privacy Osmind patients cannot depend on any of these.
What you need is a delivery method that meets the patient where they already are, in the privacy of their own home, without an app, without a portal, and without a barrier.

Curogram is a HIPAA-compliant 2-way texting platform built for medical practices. For Osmind users, the workflow for sensitive pre-treatment screening is straightforward and respectful of how patients actually behave with their phones.
The evening before a patient's appointment, Curogram sends them a text. The text contains a secure link to their screening forms — PHQ-9, GAD-7, C-SSRS, a pre-infusion safety checklist, or any combination your protocols require.
The patient taps the link. The form opens in their mobile browser. No app to install. No portal password to remember. No friction.
They complete the screening at home. Alone. At their own pace. They submit. The completed responses arrive in your team's dashboard before the patient arrives at the clinic.
Curogram handles patient-facing data collection. Osmind handles your clinical record. Your provider reviews the Curogram form responses before walking into the treatment room, then documents findings inside Osmind as they normally would.
The screening happens privately. The longitudinal tracking happens inside Osmind. The two systems do what each is best at, and your patient gets a better experience in both.
SMS works for sensitive pre-visit screening because it removes the barriers other channels add.
The patient experience comes down to a few specific attributes:
Curogram is HIPAA-compliant by design. The text itself contains no PHI. The form is delivered through a secure link that verifies the patient before showing content.
That is how patient experience digital forms ketamine clinic should look in 2026:
Simple on the surface, secure underneath.

Two things change when you move sensitive screening out of the waiting room. One is clinical. One is operational. Both matter.
The same questions, asked in private, produce more honest answers. Studies on technology-mediated assessment in psychiatry have shown reporting rate increases in the range of 20–40% for sensitive items, depending on the population.
The operational side follows naturally. A patient who completes their screening the night before arrives ready for the clinical conversation. Your team has reviewed the data. They walk in already knowing where to focus, and the infusion starts on time more often.
Consider a practice doing 200 infusions per month at an average reimbursement of $400 per visit. If pre-arrival screening shortens each visit's intake portion by 8 minutes, that frees roughly 27 hours of provider and room time per month.
Even one additional infusion per week added back from that recovered time is roughly $1,600 monthly, or $19,200 per year. That is not the primary reason to move screening home. It is a real secondary benefit.
For your team, this means cleaner data, smoother visits, and modest revenue capture from recovered time. For the patient, it means psychiatric screening patient comfort SMS delivery instead of a clipboard in a public space.
A patient with treatment-resistant depression is scheduled for their fourth ketamine infusion on a Thursday morning. On Wednesday at 6 p.m., they receive a Curogram text with a link to their PHQ-9 and C-SSRS.
They open it on the couch. They take their time. On question 9 of the PHQ-9, they mark a 2 instead of the 0 they would have marked in the waiting room. On the C-SSRS, they answer honestly about a passive thought they had last weekend.
The form lands in your dashboard at 6:18 p.m. Wednesday. A staff alert flags the C-SSRS response above your set threshold. Thursday morning, before the patient arrives, the psychiatrist already knows what to ask about.
The pre-infusion conversation includes a real safety check. Monitoring is adjusted. The infusion proceeds with the right protocol in place.
The screening did exactly what it was supposed to do. It surfaced a flag. It informed a clinical decision. It worked because the patient had privacy to be honest.
Sensitive screening is only useful when patients can answer honestly. Clipboards in waiting rooms do not give them that space. Portals and apps put a wall between the patient and the form. Email gets ignored.
A text link does not. It meets your patients in the place they already trust their phone — at home, in private, on their own time.
For Osmind practices, the impact is direct. Your longitudinal data gets more accurate, creating cleaner records for advanced analytics and scheduling decisions.
Your PHQ-9 trends actually reflect what your patients are experiencing. Safety flags surface before the patient walks in, not after. Your team starts each visit with the truth in front of them instead of a softened version of it.
The clinical case for moving sensitive screening home is straightforward. The operational case is, too. Cleaner data. Smoother visits. Patients who feel respected by the way you ask them difficult questions.
Curogram is the platform that delivers it. HIPAA-compliant SMS. No app. No portal login. Forms that open in one tap, complete in three to five minutes, and land in your dashboard before the appointment starts. It works alongside Osmind, not against it.
If you run an interventional psychiatry practice on Osmind, this is one of the lowest-friction changes you can make with one of the highest returns on clinical data quality.
Schedule a Demo with our team to see exactly how at-home pre-treatment screening Osmind patients private SMS form completion would work inside your current workflow.
💡 Digital pre-treatment screening forms Osmind interventional psychiatry SMS workflows let you send PHQ-9, GAD-7, and safety assessments through a...
💡 Clipboard intake forms slow down Osmind ketamine clinics. When 2–3 patients arrive without completed in-app assessments, staff fall back on...
💡 Interventional psychiatry patients often miss appointments because app-based reminders require effort their condition may limit. Depression,...